Page 1 of 11
SU1.1-2 | Homeostasis and Metabolic Response to Injury — SDL Guide
Learning Objectives
- Describe the concept of homeostasis and enumerate the metabolic changes that follow injury together with their mediators (SU1.1).
- Distinguish the ebb and flow phases of the metabolic response to injury and the neuroendocrine and inflammatory drivers of each (SU1.1).
- Describe the wound-related, patient-related and treatment-related factors that amplify or attenuate the metabolic response to injury (SU1.2).
INSTRUCTIONS
Every operation and every major injury triggers a stereotyped, body-wide metabolic reaction long before the wound itself begins to heal. Understanding this response is what lets a surgeon predict who will need extra fluid, who is silently catabolising muscle, and why early feeding, warmth and good analgesia genuinely change outcomes. This module builds the basic-science foundation that the rest of surgical practice — fluids, nutrition, transfusion and critical care — depends on.
References
- Bailey & Love's Short Practice of Surgery, Metabolic Response to Injury chapter (textbook)
- SRB's Manual of Surgery, Metabolic Response to Trauma (textbook)
- Sabiston Textbook of Surgery, Surgical Metabolism and Nutrition (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old man is brought in four hours after a road traffic crash with a fractured femur and a ruptured spleen. He is cold, his hands are clammy and white, his pulse is 120 and his urine output has fallen to a trickle — yet his blood pressure is still 'normal'. Over the next week, despite successful surgery, his blood sugar climbs, he loses several kilograms of muscle, and he retains litres of salt and water. None of this is random. Every one of these changes is part of a single, predictable programme the body runs after serious injury. If you can read that programme, you can anticipate his needs before the numbers swing — and that is the whole point of this module.
WHY THIS MATTERS
The metabolic response to injury sits underneath almost every decision on a surgical ward. It explains why a freshly injured patient is fluid-depleted and vasoconstricted, why blood glucose rises even in non-diabetics, why a septic or burned patient melts away lean body mass, and why salt and water are retained after major surgery. Get the model right and your fluid prescriptions, your nutrition plans and your interpretation of a falling urine output all become reasoned rather than reflexive. Get it wrong and you over-transfuse the compensating patient, starve the catabolic one, and miss the early shock that hides behind a 'normal' blood pressure. This is foundational surgical science — it is examined directly and applied every single day.
RECALL
Before going further, recall three pieces of basic physiology you already know. First, the hypothalamic-pituitary-adrenal axis: stress drives the hypothalamus and pituitary to release ACTH, which stimulates the adrenal cortex to secrete cortisol. Second, the renin-angiotensin-aldosterone system and antidiuretic hormone, which together conserve sodium and water when circulating volume falls. Third, acute inflammation from pathology: injured tissue and activated macrophages release cytokines such as IL-1, IL-6 and TNF-alpha that orchestrate the body-wide response. Keep these three systems in mind — the metabolic response to injury is essentially these familiar circuits all firing together, hard, at the same time.
Why the Body's Response to Injury Matters to the Surgeon
The metabolic response to injury is the coordinated, body-wide series of neuroendocrine, immunological and metabolic changes that follow any significant trauma — accidental or surgical, including burns, sepsis and major operations. It is best understood not as a disease but as an evolved survival programme: faced with blood loss and tissue damage, the body prioritises maintaining circulating volume, mobilising fuel, and defending against infection, even at the cost of breaking down its own tissues. For the surgeon, this matters because the response is largely predictable, broadly proportional to the size of the insult, and — crucially — modifiable. Knowing its shape lets you anticipate fluid needs, recognise concealed shock, plan nutrition, and time interventions. The magnitude of the response also serves as a rough barometer of injury severity and of how the patient is coping. Modern surgical care deliberately blunts the harmful, excessive parts of this response — through prompt resuscitation, warmth, effective analgesia, minimally invasive techniques and early enteral feeding — so that the patient retains the protective elements without paying the full catabolic price.
Provided image
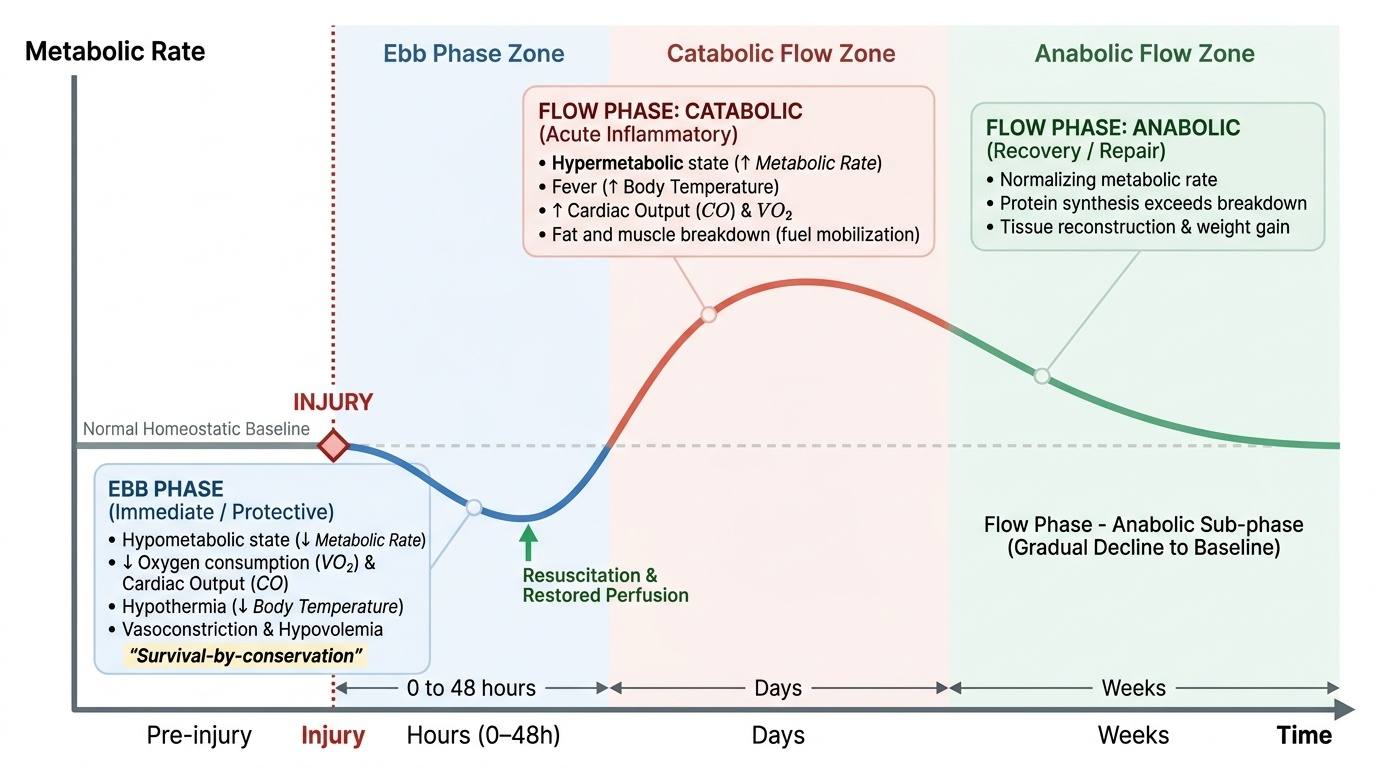
Homeostasis and the Two Phases of the Injury Response
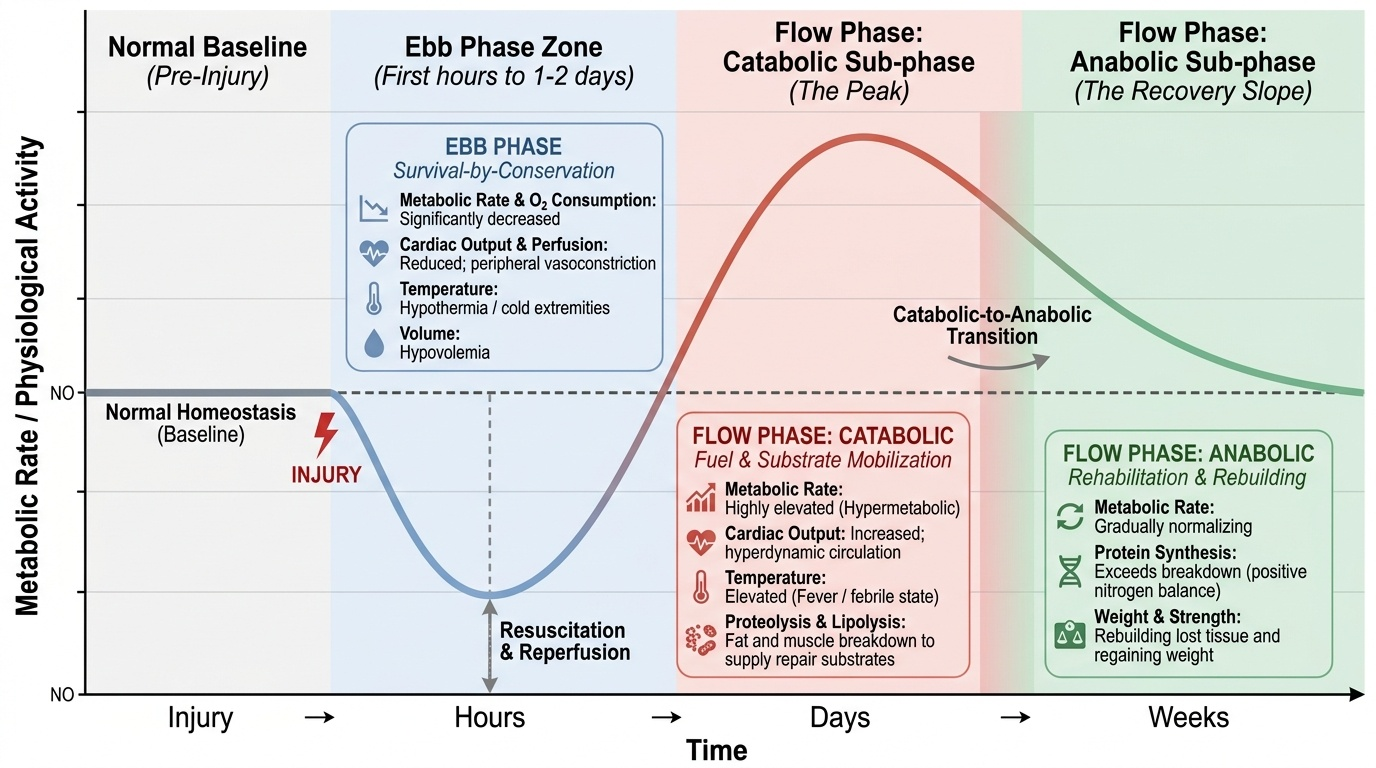
Homeostasis is the maintenance of a stable internal environment — temperature, pH, osmolality, glucose and circulating volume — within narrow limits despite external change, achieved through negative-feedback control loops. Injury is a violent challenge to homeostasis, and the body's reply unfolds in two classic temporal phases first described by Cuthbertson. The ebb phase is the immediate response, lasting roughly the first hours to a day or two: it is a hypometabolic, protective state marked by reduced metabolic rate and oxygen consumption, hypovolaemia, peripheral vasoconstriction, a tendency to hypothermia, and reduced tissue perfusion — the body 'pulling in' to preserve the central circulation. As resuscitation restores perfusion, the patient enters the flow phase, a hypermetabolic state that may last days to weeks in proportion to injury severity. The flow phase itself runs first through a catabolic sub-phase — raised metabolic rate, fever, increased cardiac output, breakdown of fat and protein to supply fuel and substrate for repair — and then, as recovery proceeds, into an anabolic sub-phase in which the patient rebuilds lost tissue and regains weight. Reading where a patient sits on this curve tells you what to expect and what to provide.
Provided image
- Ebb phase: early, short, hypometabolic; hypovolaemia, vasoconstriction, hypothermia, low cardiac output — survival-by-conservation.
- Flow phase (catabolic): hypermetabolic, febrile, raised cardiac output; fat and muscle broken down for fuel and repair substrate.
- Flow phase (anabolic): later recovery; protein synthesis exceeds breakdown, weight and strength return.
SELF-CHECK
Four hours after major trauma a patient is cold, vasoconstricted, hypovolaemic and has a reduced metabolic rate. Which phase of the metabolic response to injury does this describe?
A. The ebb phase
B. The catabolic part of the flow phase
C. The anabolic part of the flow phase
D. The convalescent (recovery) phase
Reveal Answer
Answer: A. The ebb phase
The early, short-lived state of hypometabolism, hypovolaemia, vasoconstriction and a tendency to hypothermia is the ebb phase (Cuthbertson). The hypermetabolic, febrile, catabolic flow phase follows only after resuscitation restores perfusion.
Mediators: The Neuroendocrine and Inflammatory Drivers
The phases above are produced by two interacting arms of mediators: a neuroendocrine arm and an inflammatory (cytokine) arm. The neuroendocrine arm is triggered by afferent nerve signals from the wound (pain), by hypovolaemia sensed at baroreceptors, and by changes in blood chemistry. It drives the sympathoadrenal system to release catecholamines (adrenaline and noradrenaline), producing tachycardia, vasoconstriction and glycogenolysis; it activates the hypothalamic-pituitary-adrenal axis to release cortisol, the dominant catabolic hormone that promotes gluconeogenesis, proteolysis and lipolysis and induces insulin resistance; and it raises glucagon, which together with cortisol and catecholamines forms the trio of counter-regulatory hormones that drive the characteristic post-injury hyperglycaemia. In parallel, antidiuretic hormone (ADH/vasopressin) and aldosterone are secreted to conserve water and sodium and defend circulating volume. The inflammatory arm is led by macrophage- and leucocyte-derived pro-inflammatory cytokines — chiefly IL-1, IL-6 and TNF-alpha. These produce fever, mobilise the immune response, and, through IL-6 in particular, drive the hepatic acute-phase response (rising C-reactive protein and fibrinogen, falling albumin). Together, the neuroendocrine and inflammatory arms convert a local wound into the systemic metabolic picture seen at the bedside.
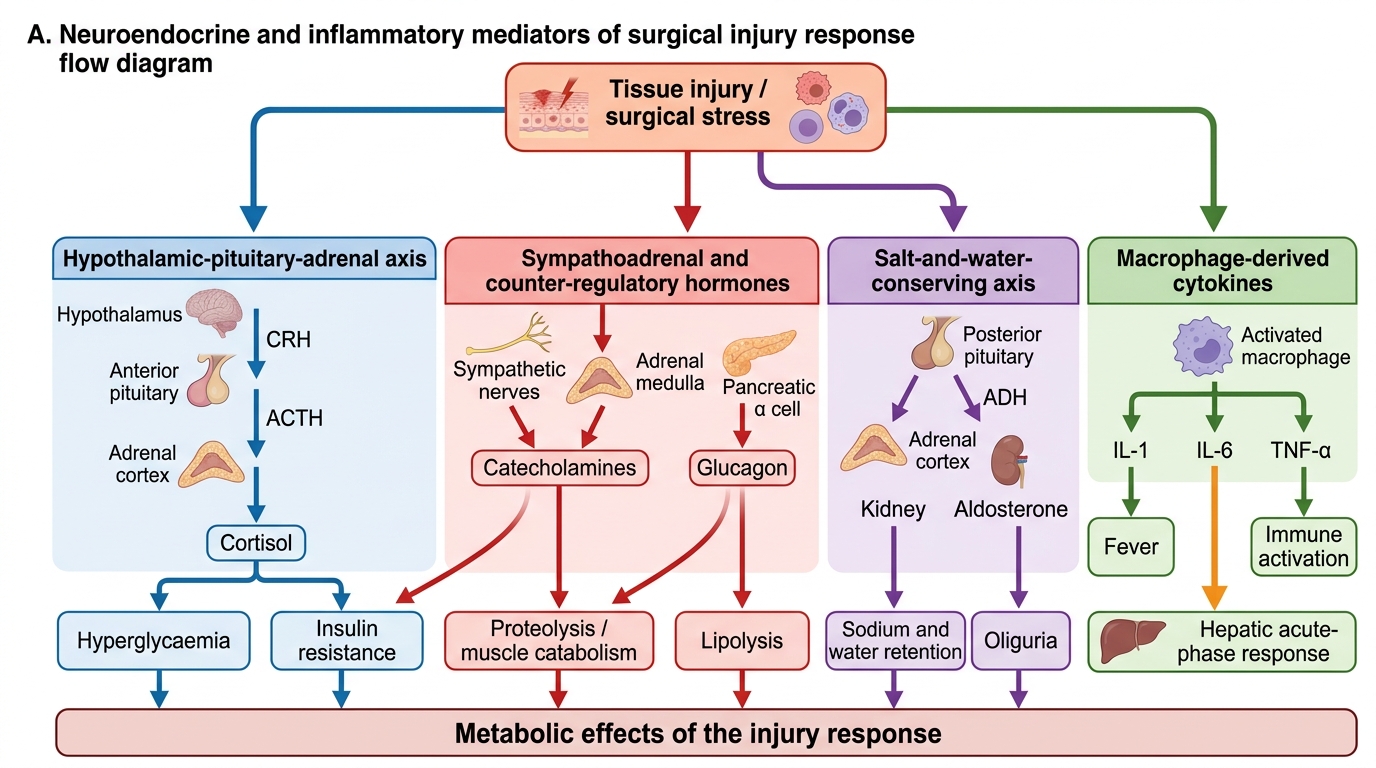
Mediators of the Surgical Injury Response
- Counter-regulatory hormones: cortisol, catecholamines, glucagon → hyperglycaemia, catabolism, insulin resistance.
- Salt-and-water-conserving axis: ADH and aldosterone → sodium and water retention, oliguria.
- Pro-inflammatory cytokines: IL-1, IL-6, TNF-alpha → fever, immune activation; IL-6 drives the hepatic acute-phase response.