Page 4 of 11
SU13.3-4 | Organ Donation Ethics and Counselling — SDL Guide
Learning Objectives
- Discuss the legal and ethical framework governing organ donation in India, including the Transplantation of Human Organs Act 1994 (amended 2011), brain-stem death, the near-relative rule and the prohibition of commercial dealing (SU13.3).
- Describe the types of organ donor and the consent and authorisation pathway, and the ethical principles of autonomy, beneficence, non-maleficence and justice as they apply to donation (SU13.3).
- Counsel patients and relatives on organ donation in a simulated environment using a structured, empathic communication approach that separates breaking bad news from the donation request and respects the family's decision (SU13.4).
INSTRUCTIONS
Every successful transplant begins with a gift — an organ given by a living donor or, far more often, by a family who agree to donation in the worst moment of their lives. Two things make that gift possible: a legal framework that keeps donation ethical and free of commerce, and the human skill of counselling a grieving family with honesty and compassion. This module gives you the law you must know and the communication routine you will practise in simulation before you ever sit with a real family. The two are inseparable: the law protects the vulnerable, and the counselling honours them.
References
- Bailey & Love's Short Practice of Surgery, Transplantation chapter (textbook)
- Transplantation of Human Organs Act 1994 (amended 2011), Government of India (statute)
- SRB's Manual of Surgery, Organ Transplantation and Medical Ethics (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is two in the morning in the intensive care unit. A 28-year-old man, declared brain-stem dead after a road traffic crash, lies ventilated and pink, his chest still rising and falling. His mother sits beside him holding his warm hand, unable to believe he is gone because he does not look dead. Somewhere else in the hospital, a young father with two children is dying of liver failure, and a teenager has spent two years on dialysis. One conversation — handled well or handled badly — stands between those waiting patients and the organs that could save them. How you speak to this grieving mother, what the law allows, and whether you can separate the terrible news of her son's death from the question of donation, will decide everything. This is not a technical skill bolted onto surgery; it is surgery's most human moment, and it can be learned.
WHY THIS MATTERS
There is a vast and permanent gap between the number of patients who need an organ and the number of organs available, and that gap costs lives every day. Closing it depends on two things you can directly influence: a sound legal and ethical framework, and skilled, compassionate counselling of potential donors and their families. As a clinician you will be the person who identifies a potential donor, who must know exactly what the law permits and forbids, and who may be asked to raise donation with a family. Get the law wrong and you risk an unethical or illegal transplant and the exploitation of the poor; get the conversation wrong and you lose both a possible donation and the family's trust. The skills here — the statute, the ethical principles, and a structured way of talking to families — are examined directly and applied in real intensive-care and transplant practice. Mastering them now, in simulation, builds the confidence and the discipline that protect both the grieving family and the patient waiting for an organ.
RECALL
Recall two things you have already learned. First, from transplant immunology: a transplant requires a donor organ matched to the recipient, and every transplant — and the lifelong immunosuppression that follows — is only possible because an organ was donated. Donation is therefore the indispensable first step of the whole transplant enterprise. Second, recall the basic principles of breaking bad news and patient-centred communication: choose a private setting, find out what the family already understands, give the news clearly and without jargon, allow silence and emotion, and respond to feelings before facts. You may already know a framework such as SPIKES. These same communication foundations underpin donation counselling — but with one critical addition you will learn here: the news of death and the request for donation must be handled as two separate conversations, not one.
Why Organ Donation Needs Both Law and Compassion
The clinical indication for understanding organ donation is simple and constant: every organ transplant depends on an organ being donated, and the supply of organs falls far short of the need, so identifying and respectfully approaching potential donors is part of good surgical and critical-care practice. Organ donation is the giving of an organ or tissue, by a living person or after death, for transplantation into another. It is unusual among clinical acts because it brings no medical benefit to the donor — a living donor accepts an operation and a deceased donor's family consents to retrieval purely for the benefit of a stranger or relative — and this asymmetry is exactly why donation must be tightly governed by law and conducted with compassion. The law exists to protect the vulnerable: to ensure consent is genuine and voluntary, to forbid the buying and selling of organs that would otherwise prey on the poor, and to define rigorously when a person on a ventilator is truly dead. Compassion exists because the families who make deceased donation possible are, almost always, in the first hours of catastrophic grief, and the way they are treated determines both whether donation happens and how they remember the death of someone they loved. This module therefore treats the legal framework and the counselling skill as two halves of one competency: the principles tell you what is permitted and right, the pathway tells you how donation proceeds, and the structured counselling approach builds the behaviour that makes an ethical donation actually possible at the bedside. Neither half works without the other.
The Legal and Ethical Framework: THOTA and the Principles of Donation
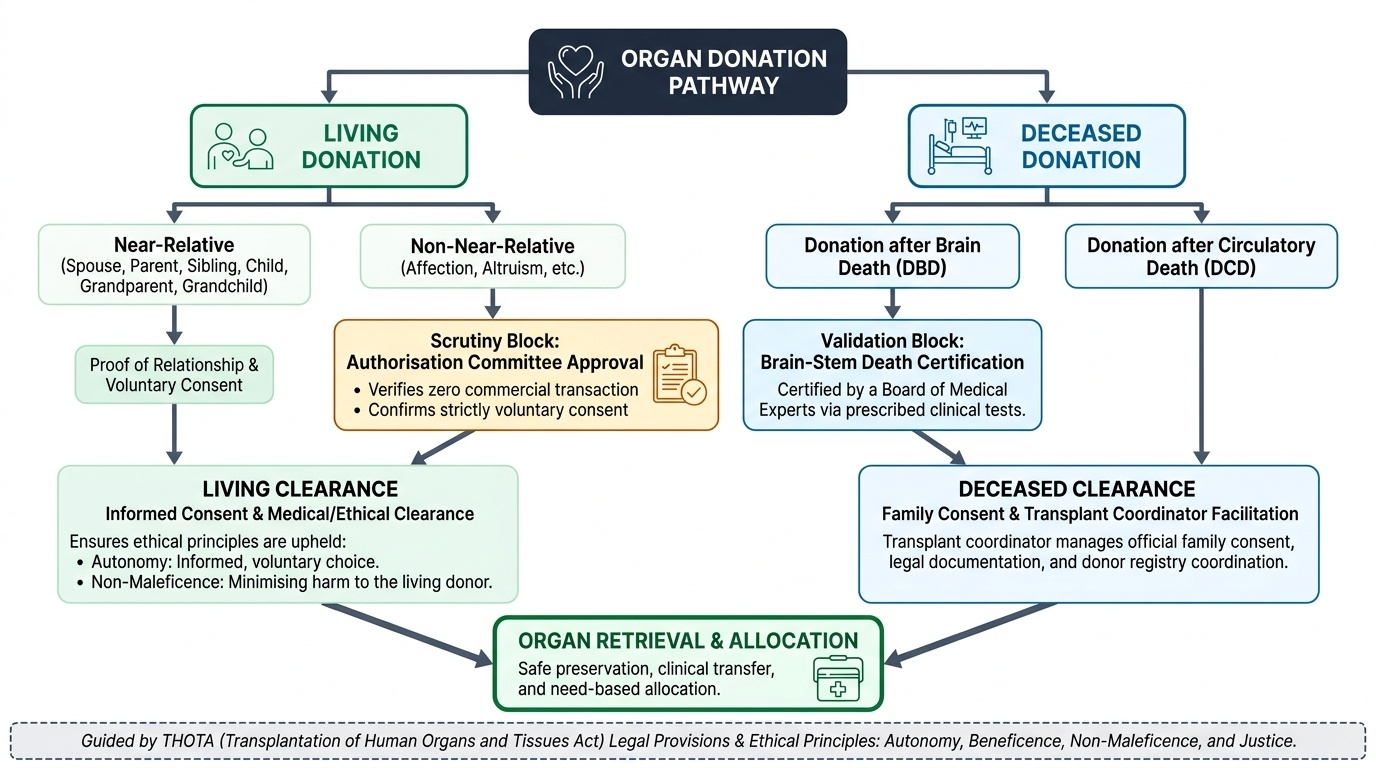
In India, organ donation and transplantation are governed by the Transplantation of Human Organs Act (THOTA), 1994, amended in 2011 (the 2011 amendment renamed it the Transplantation of Human Organs and Tissues Act and broadened its scope). You must know its core provisions. First, the Act legally recognises brain-stem death as death and lays down that it must be certified by a board of medical experts following prescribed tests — this is what makes deceased donation from a ventilated, heart-beating donor lawful. Second, the Act prohibits commercial dealing in organs: buying, selling or trading human organs is a punishable offence, the single most important safeguard against the exploitation of poor donors. Third, it regulates living donation through the concept of the near-relative. A near-relative donor — defined in the Act as spouse, son, daughter, father, mother, brother, sister, grandparent or grandchild — may donate with proof of relationship and consent without further special scrutiny. A donor who is not a near-relative (for example, out of affection or altruism) may only donate after approval by an Authorisation Committee, which exists specifically to confirm that no money has changed hands and that consent is voluntary. Fourth, the Act provides for deceased donation, including pledging and the role of the transplant coordinator. Underpinning the statute are the classical ethical principles: autonomy (genuine, informed, voluntary consent — from the donor while alive, or honouring their wishes and the family's decision after death); beneficence (the good done for the recipient); non-maleficence (minimising harm, especially to the living donor); and justice (fair, transparent and need-based allocation, not allocation by wealth). Together, statute and ethics ensure donation is a gift, never a transaction.
Provided image
Donor Types and the Donation Pathway
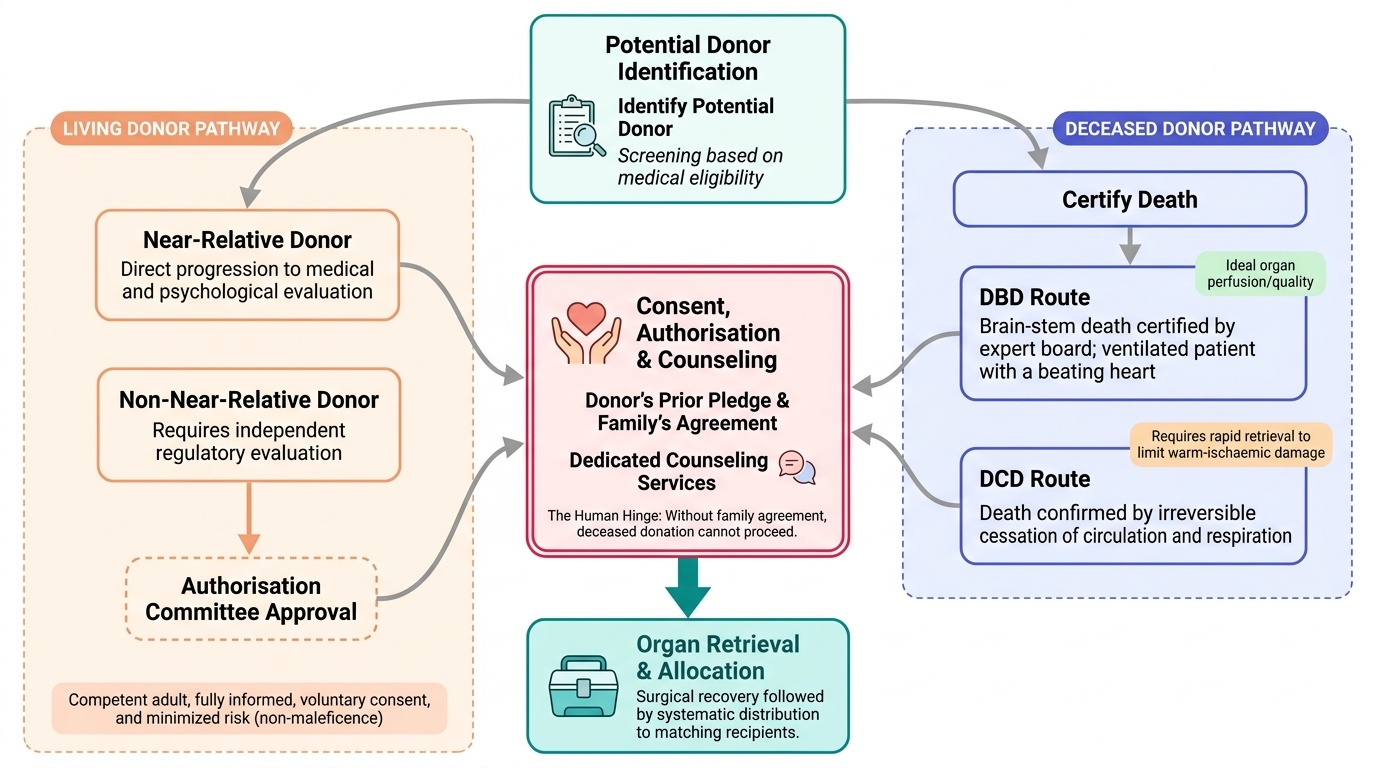
Donors fall into two broad types, and knowing the pathway for each tells you where consent, authorisation and counselling sit. A living donor gives a paired or partial organ — most commonly one kidney, or a portion of liver — while alive; this requires that the donor be a competent adult giving fully informed, voluntary consent, that they be either a near-relative or approved by the Authorisation Committee, and that the risk to them be minimised (the principle of non-maleficence). A deceased donor donates after death, and this is the source of most organs and most hearts, lungs and pancreases. Deceased donation has two routes you must distinguish. Donation after brain death (DBD) follows certification of brain-stem death in a ventilated patient whose heart is still beating and whose organs remain well-perfused — the ideal deceased-donation scenario, since organ quality is preserved. Donation after circulatory death (DCD) follows death confirmed by the irreversible cessation of circulation and respiration, after which organs must be retrieved quickly to limit warm-ischaemic damage. The donation pathway therefore runs: identify a potential donor → in deceased donation, certify death (brain-stem death by the expert board, or circulatory death) → obtain consent or authorisation (the donor's prior pledge, the family's agreement, and for non-near-relative living donors the Authorisation Committee) → and only then proceed to organ retrieval and allocation. Counselling sits at the consent step and is the human hinge of the whole pathway: without a family's agreement, a medically suitable deceased donor yields nothing. Identifying who is a potential donor early, and approaching the family well, is therefore as much a part of the pathway as the surgery itself.
Provided image
- Living donor: paired/partial organ (kidney, liver segment); competent, voluntary consent; near-relative or Authorisation-Committee-approved; minimise donor harm.
- Deceased donor — DBD: after certified brain-stem death; heart-beating, well-perfused organs; the ideal scenario.
- Deceased donor — DCD: after irreversible circulatory and respiratory arrest; rapid retrieval to limit warm ischaemia.
- Pathway: identify donor → certify death → consent/authorisation (counselling sits here) → retrieval → allocation.
SELF-CHECK
A patient wishes to donate a kidney to a friend out of pure altruism — the friend is not a spouse, parent, child, sibling or grandparent. Under the Transplantation of Human Organs Act, what is required before this donation can proceed?
A. Nothing extra — any willing adult can donate to anyone
B. Approval by an Authorisation Committee, which confirms no money has changed hands and consent is voluntary
C. Certification of brain-stem death by a board of experts
D. Payment of a regulated fee to the donor
Reveal Answer
Answer: B. Approval by an Authorisation Committee, which confirms no money has changed hands and consent is voluntary
Because the friend is not a near-relative (spouse, son, daughter, father, mother, brother, sister, grandparent or grandchild), the living donation can only proceed after an Authorisation Committee approves it. The Committee exists to confirm the donation is genuinely altruistic and voluntary and that no commercial dealing — which the Act prohibits — is involved. Brain-stem death certification applies to deceased, not living, donation, and paying a donor is illegal.