Page 1 of 16
SU14.{1,4} | Asepsis, Sterilization and Surgical Field Practice — SDL Guide
Learning Objectives
- Describe the principles of aseptic technique, sterilization and disinfection, including the Spaulding classification (SU14.1).
- Describe the physical and chemical methods of sterilization with their standard parameters, and how a sterile field is established and maintained (SU14.1).
- Demonstrate asepsis — surgical scrubbing, gowning, gloving and field maintenance — and basic suturing in a simulated environment (SU14.4).
INSTRUCTIONS
Surgical site infection is one of the most common and most preventable harms in surgery, and almost all of its prevention happens before and during the operation through disciplined asepsis. This module gives you the vocabulary, the science of sterilization, and the hands-on routine of scrub, gown, glove and sterile-field practice — the everyday skills that separate a safe operating theatre from a dangerous one. You will practise these in simulation before you ever take them to a real patient.
References
- Bailey & Love's Short Practice of Surgery, Surgical Infection and Asepsis (textbook)
- SRB's Manual of Surgery, Sterilization, Asepsis and Antisepsis (textbook)
- Sabiston Textbook of Surgery, Surgical Infections and Choice of Antibiotics (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients have the same clean operation on the same day in the same theatre. One goes home on the third day, the wound healing cleanly. The other returns a week later with a red, discharging wound, spends extra days in hospital on antibiotics, and carries a scar — and a fear of surgery — for life. The operation was identical; what differed was the chain of asepsis around it. A glove perforated and not changed, an instrument reprocessed at the wrong level, a sterile field broken by a careless reach across the trolley — any one of these can decide the outcome. Asepsis is not a ritual; it is the most powerful, cheapest infection-prevention tool a surgeon has, and it is entirely in your hands.
WHY THIS MATTERS
Surgical site infection prolongs hospital stay, raises cost, occasionally kills, and is overwhelmingly preventable. The single largest lever is aseptic technique — keeping the operative field free of microorganisms by combining correctly sterilized instruments, properly disinfected skin and a disciplined sterile field. As a clinician you will reprocess and select equipment, scrub and gown for procedures, and supervise others doing the same; getting the principles right protects every patient you touch. The skills here are also examined directly and are a prerequisite to ever operating: no one is allowed near a sterile field until they can scrub, gown and glove without contaminating themselves. Mastering this now, in simulation, builds the muscle memory that keeps patients safe later.
RECALL
Recall the microbiology that underpins this skill. From MI: microorganisms include vegetative bacteria, the far more resistant bacterial spores, fungi, viruses and prions, and any process claiming to 'sterilize' must destroy even spores. Recall too that moist heat kills by coagulating proteins and is more efficient than dry heat at the same temperature, which is why steam under pressure is the workhorse of the theatre. From your surgical-infection learning, recall the determinants of surgical site infection — the dose and virulence of the contaminating organism set against host resistance — and the wound classification (clean, clean-contaminated, contaminated, dirty). Asepsis is how we drive the contaminating dose towards zero.
Why Asepsis Decides the Outcome of an Operation
The clinical indication for rigorous asepsis is every invasive procedure, because every breach risks a surgical site infection (SSI) — infection of the tissues handled during an operation. The logic is simple and quantitative: infection results when the contaminating microbial dose and virulence overwhelm host resistance, and asepsis is the deliberate minimisation of that dose at the operative field. Most SSIs are acquired in theatre from the patient's own flora, the surgical team, the instruments or the environment, and most are preventable by sound technique. This is why asepsis — keeping an area free of microorganisms — is the central discipline of the operating theatre, supported by correct sterilization of instruments, disinfection and antisepsis of skin, and a maintained sterile field. Understanding the relevance also frames the rest of this module: the definitions and the Spaulding principle tell you what level of decontamination each item needs, the methods tell you how to achieve it, the monitoring tells you whether it worked, and the simulated practice builds the behaviour that keeps the field clean during a real operation. A single weak link — an under-reprocessed scope, a soaked drape, an unnoticed glove tear — can undo all the rest.
Core Definitions and the Spaulding Principle
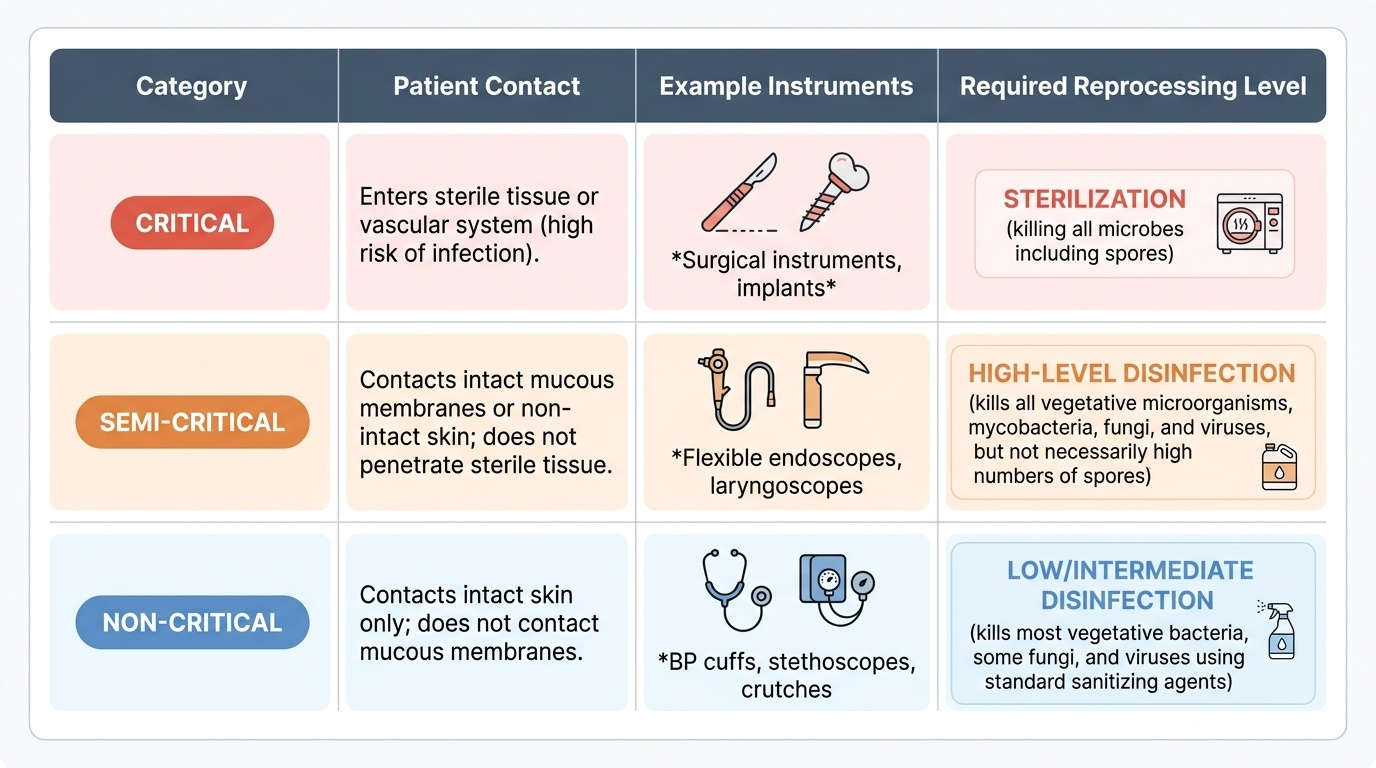
Precise terms prevent dangerous shortcuts, so learn them exactly. Sterilization is the destruction or removal of all microbial life, including the highly resistant bacterial spores. Disinfection is the removal of most pathogenic microorganisms from inanimate surfaces but does not reliably kill spores; high-level disinfection kills all microbes except large numbers of spores. Antisepsis is disinfection applied to living tissue — the skin and mucous membranes — using agents such as chlorhexidine or povidone-iodine. Asepsis is the overarching goal: a state or technique that keeps an area free of microorganisms. The governing framework that tells you which level any reusable item requires is the Spaulding classification, which ranks devices by the infection risk of their intended use. Critical items enter sterile tissue or the vascular system (surgical instruments, implants) and must be sterilized. Semi-critical items contact intact mucous membranes but do not penetrate sterile tissue (flexible endoscopes, laryngoscope blades) and require at least high-level disinfection. Non-critical items contact only intact skin (blood-pressure cuffs, stethoscopes) and need only low- or intermediate-level disinfection. Matching the item to its Spaulding category is the single most important reprocessing decision.
Provided image
| Spaulding category | Contact | Example | Required reprocessing |
|---|---|---|---|
| Critical | Enters sterile tissue / vascular system | Surgical instruments, implants | Sterilization |
| Semi-critical | Contacts intact mucosa | Flexible endoscopes, laryngoscope blades | High-level disinfection |
| Non-critical | Contacts intact skin only | BP cuff, stethoscope | Low/intermediate-level disinfection |
SELF-CHECK
Under the Spaulding classification, a reusable surgical instrument that enters sterile tissue is a 'critical' item. What is the minimum required level of reprocessing?
A. Cleaning with detergent only
B. Low-level disinfection
C. High-level disinfection
D. Sterilization
Reveal Answer
Answer: D. Sterilization
Critical items penetrate sterile tissue or the vascular system and must be STERILIZED — destroying all microbes including spores. High-level disinfection is the minimum for semi-critical items (mucosal contact), and low/intermediate-level disinfection suffices for non-critical items (intact skin only).
Sterilization and Disinfection Techniques
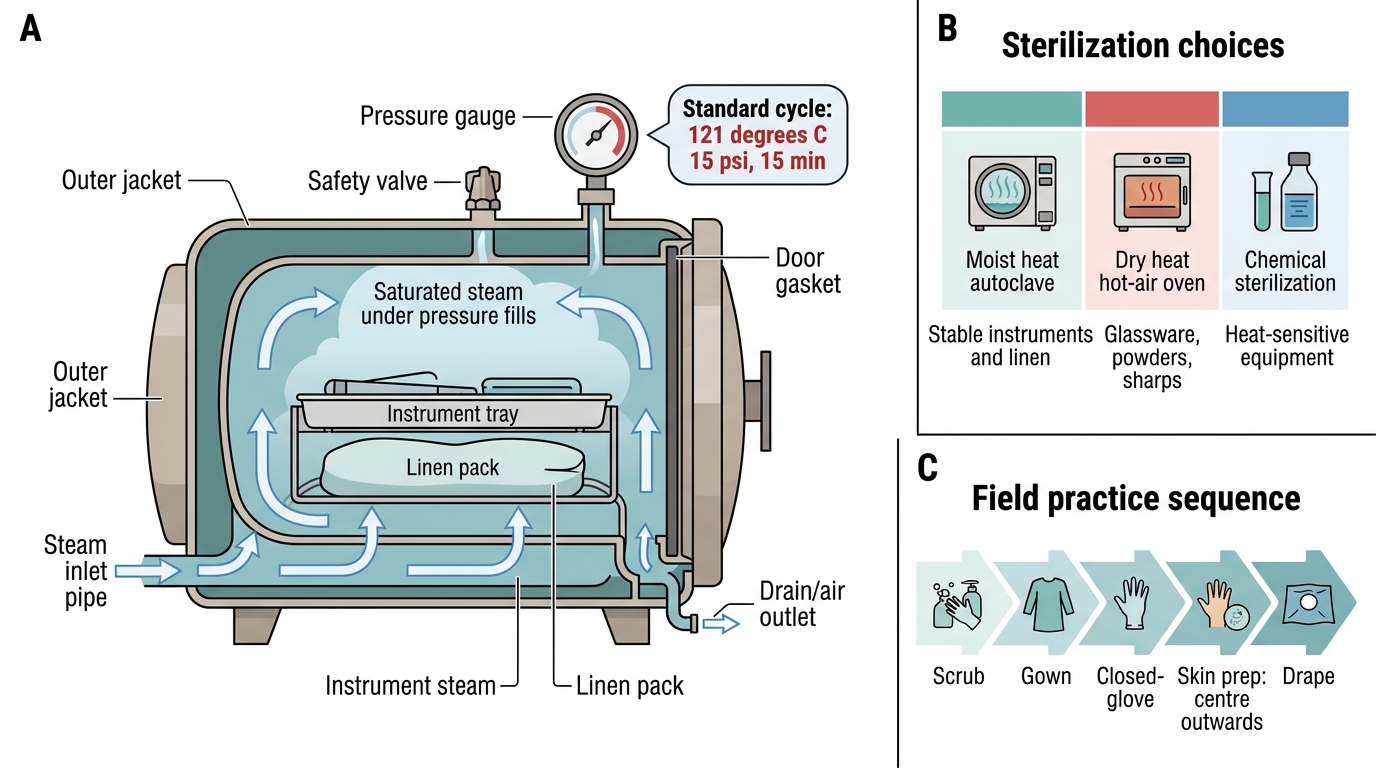
Sterilization methods are grouped as physical and chemical, and you choose by what the item can tolerate. The theatre workhorse is moist-heat sterilization in the autoclave, which uses saturated steam under pressure: the standard cycle is 121 degrees C at 15 psi for 15 minutes (a higher-temperature 'flash' cycle runs at about 134 degrees C for around 3 minutes). Moist heat coagulates microbial proteins and reliably kills spores, making it first choice for heat- and moisture-stable instruments and linen. Dry-heat sterilization in a hot-air oven (typically 160 degrees C for 1–2 hours) suits items damaged by moisture, such as glassware, powders and sharp instruments. Filtration sterilizes heat-labile fluids, and ionising radiation is an industrial method for single-use disposables. For heat-sensitive equipment, chemical sterilization with ethylene oxide gas or glutaraldehyde / hydrogen-peroxide plasma is used. Establishing the sterile field then layers on top of sterile instruments: surgical hand antisepsis (a timed scrub with chlorhexidine or povidone-iodine, or an alcohol-based hand rub), donning a sterile gown and gloves (closed-gloving technique keeps the hands inside the cuff until gloved), skin preparation painted from the incision site outwards in concentric circles and never carried back over a cleaned area, and draping to isolate the operative field.
Steam Autoclave and Basic Sterilization Practice
- Moist heat (autoclave): 121 degrees C / 15 psi / 15 min — kills spores; first choice for stable instruments and linen.
- Dry heat (hot-air oven): ~160 degrees C / 1–2 h — glassware, powders, sharps.
- Chemical: ethylene oxide, glutaraldehyde, hydrogen-peroxide plasma — heat-sensitive equipment.
- Field practice: scrub → gown → closed-glove → skin prep (centre outwards) → drape.