Page 8 of 16
SU15.1,SU16.1 | Hospital Waste Disposal and Minimally Invasive Surgery — SDL Guide
Learning Objectives
- Describe the classification of hospital (biomedical) waste and the appropriate methods of disposal under the Indian Biomedical Waste Management Rules 2016, including the colour-coded segregation system (SU15.1).
- Describe minimally invasive general surgery — its definition, the carbon-dioxide pneumoperitoneum that makes it possible, and its indications (SU16.1).
- Describe the advantages and disadvantages of minimally invasive general surgery and judge when it is appropriate (SU16.1).
INSTRUCTIONS
Two practical pillars of modern surgical care sit alongside the operation itself: what happens to the waste it generates, and how technology lets us operate through tiny incisions instead of large ones. Mishandled hospital waste injures staff, spreads infection and harms the environment, and its safe disposal is governed by law; minimally invasive surgery has transformed patient recovery but brings its own physiology and risks. This module gives you the colour-coded system for segregating biomedical waste under the BMW Rules 2016, and the principles of minimally invasive surgery — how it works, when it is used, and what it trades off — so you can handle waste safely and reason about the surgical approach a patient is offered.
References
- Bailey & Love's Short Practice of Surgery, Minimally Invasive and Bariatric Surgery (textbook)
- SRB's Manual of Surgery, Biomedical Waste Management and Laparoscopic Surgery (textbook)
- Biomedical Waste Management Rules 2016 (and amendments), Ministry of Environment, Forest and Climate Change, Government of India (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A house officer finishes a dressing, and without thinking drops the used needle into the ordinary black bin and recaps another out of habit. Hours later a cleaner empties that bin by hand and is jabbed through the glove by the protruding needle — a single careless act that now means months of anxiety, blood tests and post-exposure prophylaxis against hepatitis B, hepatitis C and HIV. The same hospital, two floors up, removes a gallbladder through four keyhole incisions; the patient walks to the bathroom the same evening and goes home the next morning. These two scenes capture the bookends of safe modern surgery: disposing of what an operation produces without harming anyone, and operating through the smallest possible wound. Both are learnable systems, not luck — and both are your responsibility from your very first day on the wards.
WHY THIS MATTERS
How a hospital deals with its biomedical waste and whether it can offer minimally invasive surgery affect every patient and every member of staff. Mismanaged waste — a needle in the wrong bin, infected tissue mixed with general rubbish — causes needle-stick injuries, transmits blood-borne viruses, spreads infection into the community and pollutes the environment, which is why its segregation and disposal are governed by law that you must follow from day one. Minimally invasive surgery, meanwhile, has changed what recovery looks like for millions of patients, turning operations that once meant a week in hospital into day-case procedures — but it is not free of cost or risk, and knowing its trade-offs lets you counsel patients honestly. As a clinician you will personally segregate sharps and contaminated waste at the point of use, and you will discuss with patients whether an open or a keyhole operation suits them. These are examined, everyday competencies, not optional extras.
RECALL
Recall the infection-control and physiology you have already met. From su11-asepsis and your microbiology learning, recall that contaminated items carry living, sometimes blood-borne, pathogens — hepatitis B, hepatitis C and HIV among them — and that breaking the skin (a needle-stick) is a direct route of transmission; safe waste handling is simply infection control continued after the procedure. Recall too the standard precaution that needles are never recapped, because most needle-stick injuries happen during recapping. From PY, recall basic cardiorespiratory physiology: raised pressure inside the abdomen presses on the inferior vena cava and the diaphragm, and absorbed carbon dioxide must be cleared by the lungs — facts that explain why insufflating the abdomen with CO2 for keyhole surgery has measurable effects on venous return and on blood carbon-dioxide levels. These prior ideas are the foundation for both halves of this module.
Why Waste Disposal and Minimally Invasive Surgery Matter
The indication for understanding both topics is constant and practical: every clinical encounter generates waste that can injure or infect, and a growing proportion of operations are now offered as keyhole procedures, so you will meet both on every surgical attachment. Biomedical waste is any waste generated during the diagnosis, treatment or immunisation of patients — including human tissue, blood-soaked materials, sharps, contaminated plastics and expired drugs — and it is hazardous precisely because it carries live pathogens and physical danger. Handling it wrongly causes needle-stick injuries and the transmission of blood-borne viruses to staff, waste-handlers and the public, spreads hospital-acquired infection, and damages the environment; handling it correctly, by segregating it at the point of generation into the right container, neutralises almost all of that risk before it can occur. Minimally invasive surgery (MIS) — operating through small incisions with a camera and long instruments rather than through one large wound — is relevant for the opposite reason: it reduces the harm of the operation itself, giving less pain, smaller scars and faster recovery, while introducing new considerations of cost, skill and the physiology of working inside an inflated abdomen. The module is organised so that each topic moves from principle to practice: for waste, from why segregation matters, to the rules that govern it, to the colour-coded categories you physically use, to applying it safely; and for MIS, from what it is and how the CO2 pneumoperitoneum works, to weighing its advantages and disadvantages, to recognising the set-up in theatre. Both end in the same place — competent, safe behaviour around real patients.
Principles of Biomedical Waste Segregation
The governing principle of all waste management is segregation at source — separating waste into the correct category at the very moment and place it is produced, never sorting it later. This matters because once different waste types are mixed, the whole mixture must be treated as the most hazardous component, multiplying cost and risk; and because the person at the point of use is the only one who reliably knows what an item is and how contaminated it is. In India this is mandated by the Biomedical Waste Management Rules 2016 (made under the Environment (Protection) Act and subsequently amended), which require every healthcare facility to segregate waste at source into clearly labelled, colour-coded containers, each marked with the international biohazard symbol, and to treat each category by a prescribed method before final disposal. The Rules rest on a few non-negotiable behaviours: put each item in its designated colour immediately; never recap, bend or break needles, and drop sharps straight into a puncture-proof container; do not overfill containers (the three-quarters rule); keep containers labelled and within reach where waste is generated; and protect waste-handlers with training and personal protective equipment. The categories themselves are defined by what the waste is and how it must be treated — anatomical and infectious waste must be destroyed, recyclable plastics must be disinfected then recycled, and sharps must be rendered both non-infectious and non-injurious. Understanding this logic — match the item to the colour, and the colour to the treatment — is what makes the detailed table that follows easy to use rather than memorise blindly.
Colour Coding and Disposal under the BMW Rules 2016
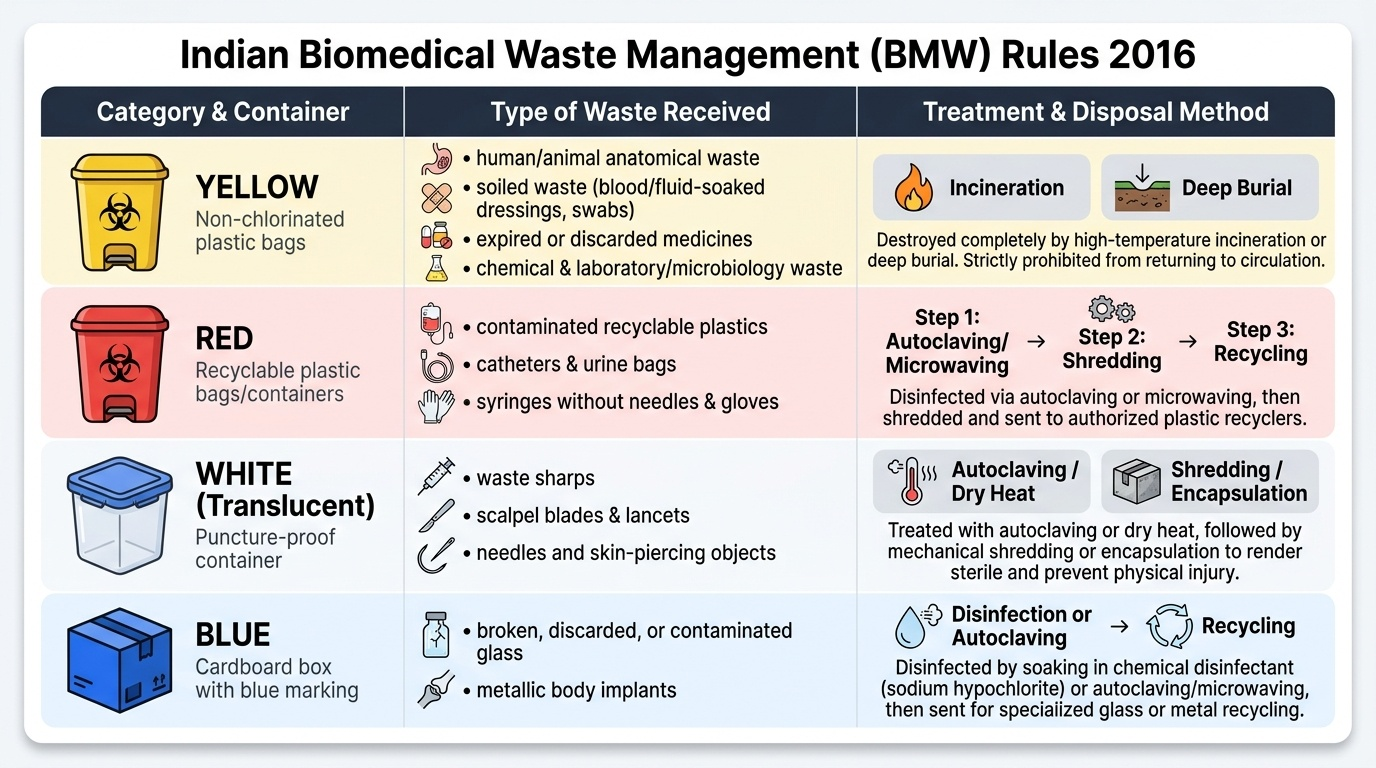
The practical heart of biomedical waste management is the colour-coded segregation system, and you must be able to assign any item to the correct bin and state how that bin is treated. There are four working colours under the BMW Rules 2016. The yellow category receives human and animal anatomical waste (tissues, organs, body parts), soiled waste (items soaked with blood or body fluids, dressings, swabs), expired or discarded medicines, chemical waste and laboratory/microbiology waste; this category is destroyed by incineration or deep burial, because it must not return to circulation. The red category receives contaminated recyclable plastic — intravenous tubing and sets, catheters, urine bags, syringes without needles, and gloves; it is autoclaved or microwaved to disinfect it, then shredded and recycled. The white (translucent), puncture-proof container receives sharps — used needles, scalpel blades, lancets and any sharp that can pierce skin; sharps are autoclaved or treated by dry heat, then shredded or encapsulated so they are both sterile and unable to injure. The blue category receives broken, discarded or contaminated glass and metallic body implants; it is disinfected (autoclaved/chemically treated) and then recycled. The single most important rule embedded in this system is for sharps: they go only into the rigid white puncture-proof container, never into a bag, and needles are never recapped. Matching the waste to its colour, and remembering the treatment method for each, is the everyday skill this competency demands.
Provided image
| Colour | Waste it receives | Treatment / disposal |
|---|---|---|
| Yellow | Anatomical/human-tissue waste, soiled waste, expired medicines, chemical and laboratory/microbiology waste | Incineration or deep burial |
| Red | Contaminated recyclable plastic — IV sets, tubing, catheters, urine bags, gloves | Autoclave/microwave, then shred and recycle |
| White (translucent, puncture-proof) | Sharps — needles, scalpel blades, lancets | Autoclave/dry heat, then shred or encapsulate |
| Blue | Broken/contaminated glass and metallic body implants | Disinfect/autoclave, then recycle |
SELF-CHECK
Under the Indian Biomedical Waste Management Rules 2016, into which container must a used hypodermic needle be discarded?
A. Yellow bag
B. Red bag
C. White (translucent) puncture-proof container
D. Blue container
Reveal Answer
Answer: C. White (translucent) puncture-proof container
Sharps such as used needles and scalpel blades go into the WHITE translucent, puncture-proof container — and the needle is never recapped. The yellow bag is for anatomical/soiled/chemical and lab waste, the red bag for contaminated recyclable plastics, and the blue container for broken glass and metallic implants.