Page 7 of 20
SU17.4-6 | Head Injury Assessment and Management — SDL Guide
Learning Objectives
- Describe the mechanisms and pathophysiology of head injury, including primary versus secondary brain injury and the intracranial haematomas (SU17.4).
- Describe the clinical features and the neurological assessment of a head-injured patient, including the Glasgow Coma Scale (SU17.5).
- Choose appropriate investigations and discuss the principles of management of head injury (SU17.6).
INSTRUCTIONS
Head injury is a leading cause of death and lifelong disability in young people, and India's roads make it an everyday emergency. The cruel feature of brain trauma is that the damage done at the instant of impact cannot be undone — but a second wave of damage, caused by low oxygen, low blood pressure and rising pressure inside the skull in the hours that follow, is largely preventable. The whole discipline of head-injury care is built around that distinction: resuscitate, assess accurately with the Glasgow Coma Scale, image the right patients, and relentlessly prevent secondary injury while deciding who needs surgery. This module takes you through that pathway from impact to definitive management.
References
- Bailey & Love's Short Practice of Surgery, Neurosurgery — Head Injuries (textbook)
- SRB's Manual of Surgery, Head Injury (textbook)
- Advanced Trauma Life Support (ATLS) Student Course Manual, American College of Surgeons — Head Trauma (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young man is brought to casualty after falling from his motorcycle. He is awake, talking, complaining only of a headache and a sore scalp; his examination seems unremarkable and a junior is ready to send him home with advice. An hour later the nurse calls you urgently — he has become drowsy, then unresponsive, one pupil is now larger than the other, and his pulse is slowing while his blood pressure climbs. In the time it took to fill in a form, an artery torn beneath his skull has been quietly bleeding, and the rising clot is now crushing his brain. This is the patient every textbook warns about — the one who 'talks and deteriorates' — and the difference between his living and dying is whether the team understood that an alert head-injured patient can still be carrying a lethal, treatable bleed.
WHY THIS MATTERS
Head injury is among the commonest reasons trauma patients die or survive with permanent disability, and most of those patients first present to a general doctor, not a neurosurgeon. The decisions made in the first hour — securing the airway, maintaining blood pressure and oxygenation, scoring the conscious level accurately, imaging the right patients and recognising deterioration — determine outcome far more than anything that happens later. Crucially, much of the brain damage after head injury is secondary and preventable, which means a well-trained first responder genuinely saves brain. As a clinician you must be able to assess a head injury reliably, communicate it in a common language (the Glasgow Coma Scale), know when to order a CT and when to refer, and never be lulled by an apparently well patient. These are core, examinable competencies for every graduate, because head-injured patients arrive everywhere and the early management is general, not specialist.
RECALL
Recall the relevant anatomy and physiology. From AN: the brain is wrapped in three meninges — the tough outer dura mater, the arachnoid, and the pia — and the middle meningeal artery runs between the skull and the dura, vulnerable to a fracture of the thin temporal bone (the key to extradural bleeding). Recall that the brain sits in a rigid, closed box; the Monro-Kellie doctrine states that the volume of brain, blood and cerebrospinal fluid inside the skull is fixed, so once compensation is exhausted, any added volume — a haematoma or swelling — raises the intracranial pressure (ICP) sharply. Recall from physiology that the brain depends on adequate cerebral perfusion (which falls if blood pressure drops or ICP rises) and on a continuous oxygen supply, so hypotension and hypoxia are direct enemies of the injured brain. Hold on to these, because they explain both why secondary injury happens and why prevention works.
The Head-Injured Patient
Head injury covers a spectrum from a trivial scalp laceration to a fatal brain crush, and the clinician's task is to identify, within that spectrum, the patient whose brain is in danger. Most head injuries follow a recognisable mechanism — road traffic crashes, falls, assaults and sports injuries — and the energy and direction of the impact predict the pattern of damage. Clinically, head injuries are graded by conscious level into mild, moderate and severe using the Glasgow Coma Scale (detailed later), and the presentation ranges from a fully alert patient with headache and a scalp wound, through confusion, vomiting, a brief loss of consciousness and amnesia (concussion), to a deeply comatose patient with abnormal pupils and posturing. The single most dangerous presentation to understand from the outset is the 'talk-and-deteriorate' patient: someone who is conscious and even lucid on arrival but then declines, because an expanding intracranial haematoma — classically an extradural bleed — takes time to accumulate before it compresses the brain. This is why a normal initial appearance must never be taken as reassurance, and why repeated reassessment is built into every head-injury protocol. Warning features that mark a head injury as serious include a falling conscious level, a worsening or severe headache, repeated vomiting, a seizure, focal neurological signs (limb weakness, an unequal pupil), and signs of a skull-base fracture (CSF leak from nose or ear, periorbital or mastoid bruising). Recognising the at-risk patient early is the first and most important step.
Head Injury: From Concussion to Coma
Mechanism and Pathophysiology — Primary, Secondary Injury and the Haematomas
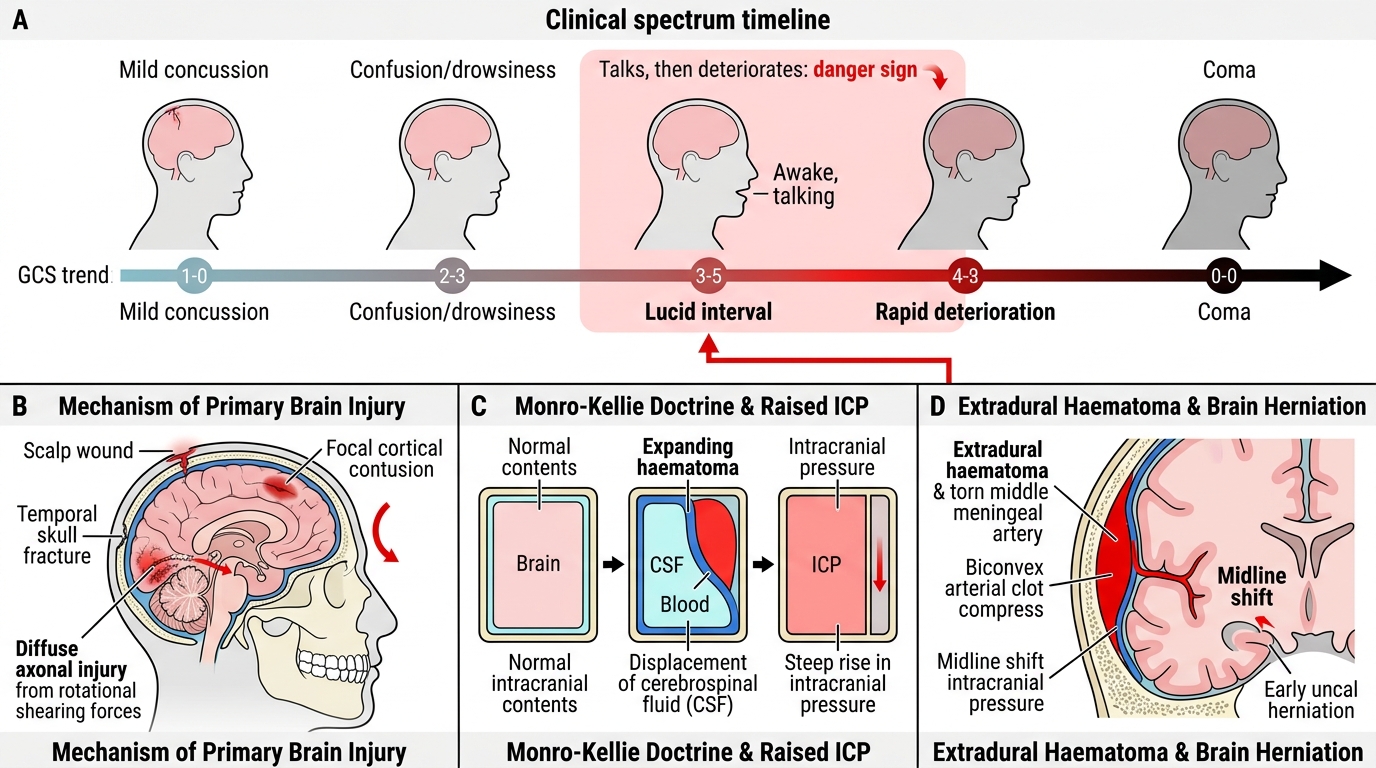
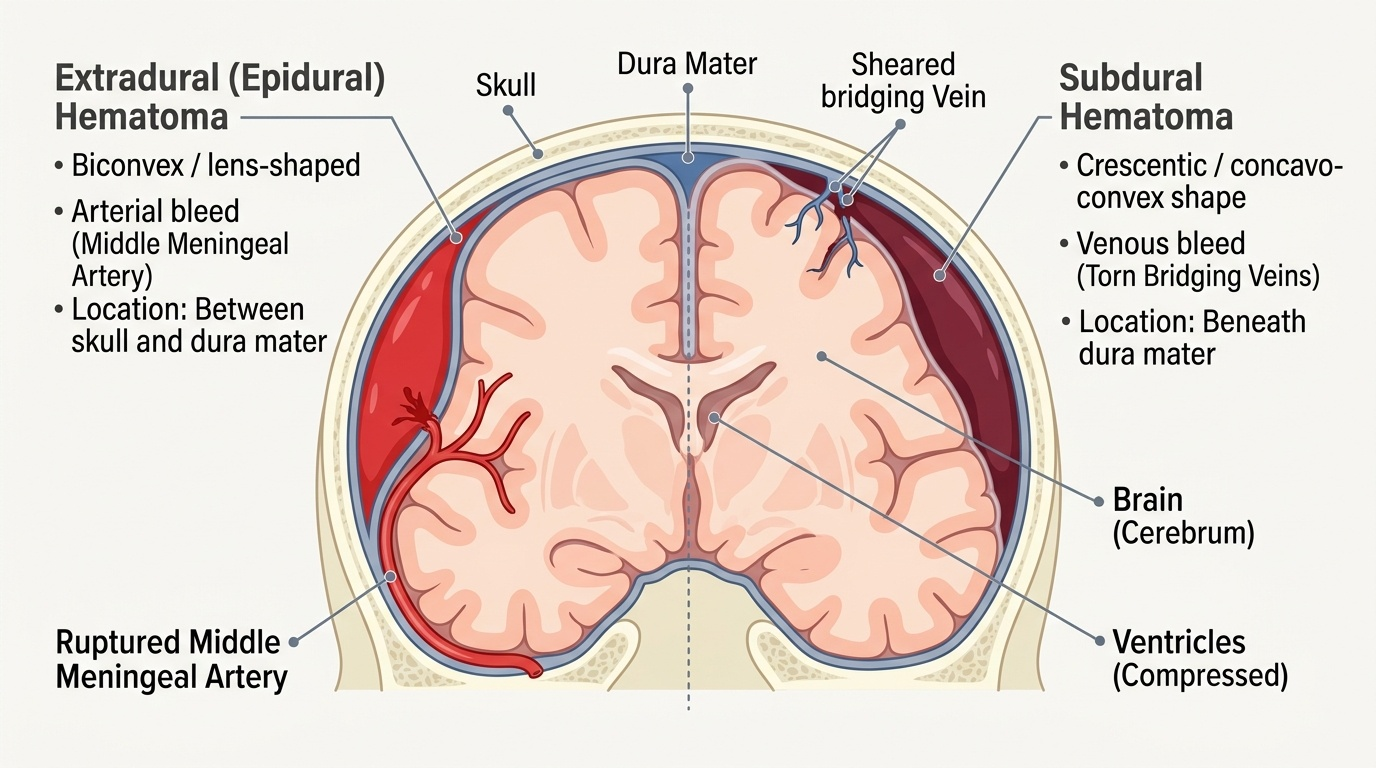
The pathophysiology of head injury rests on one organising distinction. Primary brain injury is the damage inflicted at the instant of impact — scalp and skull injury, cortical contusions, lacerations, and diffuse axonal injury (widespread shearing of nerve fibres from rotational forces). Primary injury is, by definition, already done and largely irreversible; it can only be prevented before the event (helmets, seatbelts). Secondary brain injury is the further damage that develops in the minutes to days afterwards from physiological insults — chiefly hypoxia, hypotension, raised intracranial pressure, ischaemia, hypercapnia, seizures and fever — and this is what good management exists to prevent. Because the skull is a closed box (Monro-Kellie doctrine), an expanding mass or swelling first displaces CSF and venous blood and then, once that compensation is exhausted, causes a steep rise in intracranial pressure (ICP), falling cerebral perfusion, ischaemia and ultimately herniation of brain tissue. The mass lesions that cause this are the intracranial haematomas, which you must be able to distinguish. An extradural (epidural) haematoma is an arterial bleed, usually from a torn middle meningeal artery after a temporal skull fracture; blood collects between skull and dura, producing a biconvex (lens-shaped) clot on CT and the classic lucid interval (a transient recovery of consciousness before deterioration). A subdural haematoma is a venous bleed from torn bridging veins between the brain surface and the dura, forming a crescentic (concavo-convex) collection on CT; it is common in the elderly and in those on anticoagulants and may be acute or chronic. Subarachnoid and intracerebral haemorrhages complete the group. Each can raise ICP and demand urgent recognition.
Provided image
- Primary injury (at impact, irreversible): contusion, laceration, diffuse axonal injury.
- Secondary injury (later, PREVENTABLE): hypoxia, hypotension, raised ICP, ischaemia, seizures, fever.
- Extradural haematoma: arterial (middle meningeal artery), biconvex/lens-shaped, classic lucid interval.
- Subdural haematoma: venous (bridging veins), crescentic; common in elderly/anticoagulated; acute or chronic.
SELF-CHECK
A patient with a temporal skull fracture has a biconvex (lens-shaped) clot on CT and gave a history of briefly regaining consciousness before deteriorating. Which haematoma and bleeding source does this describe?
A. Subdural haematoma from torn bridging veins
B. Extradural haematoma from the middle meningeal artery
C. Subarachnoid haemorrhage from a berry aneurysm
D. Intracerebral haematoma from a contusion
Reveal Answer
Answer: B. Extradural haematoma from the middle meningeal artery
An extradural (epidural) haematoma is an arterial bleed, classically from a torn middle meningeal artery after a temporal fracture; it appears biconvex/lens-shaped on CT and may produce a lucid interval before deterioration. A subdural haematoma is venous (bridging veins) and crescentic on CT.
Neurological Assessment — GCS, Pupils and Signs of Raised ICP
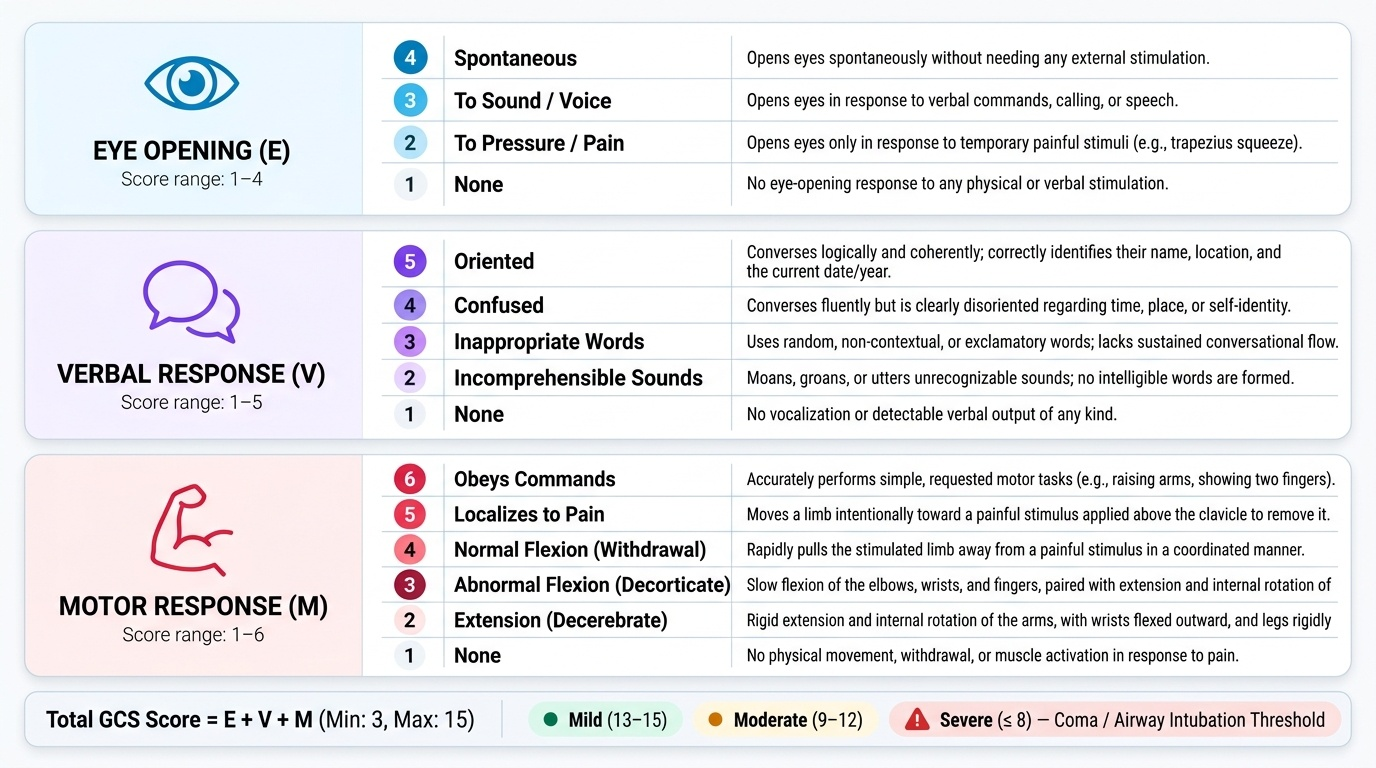
Accurate, repeatable neurological assessment is the backbone of head-injury care, and its common language is the Glasgow Coma Scale (GCS). The GCS scores three responses: Eye opening out of 4 (4 spontaneous, 3 to voice, 2 to pain, 1 none), Verbal response out of 5 (5 oriented, 4 confused, 3 inappropriate words, 2 incomprehensible sounds, 1 none), and Motor response out of 6 (6 obeys commands, 5 localises to pain, 4 normal flexion/withdrawal, 3 abnormal flexion, 2 extension, 1 none). The total therefore ranges from a maximum of 15 to a minimum of 3 (never zero), and it grades severity: mild 13-15, moderate 9-12, severe 8 or less. A GCS of 8 or less defines coma and severe head injury and is the threshold at which the airway must be secured by intubation, because such a patient cannot protect their own airway. The GCS is recorded as its three components, not just the total, and — most importantly — it is repeated serially, since a falling GCS is the earliest sign of an expanding lesion. Alongside the GCS, examine the pupils (a fixed, dilated pupil on one side suggests uncal herniation compressing the third nerve, usually on the side of an expanding clot) and look for lateralising signs such as limb weakness. Finally, recognise the Cushing reflex, the body's ominous response to dangerously raised ICP: hypertension, bradycardia and irregular (depressed) respiration — a late, pre-terminal sign demanding immediate action. The investigation of choice to find the structural cause is a non-contrast CT (NCCT) scan of the head, the first-line imaging that rapidly demonstrates haematomas, fractures, contusions and brain swelling and guides surgery; plain skull X-rays have little role in modern practice.
Provided image
| Response | Score | Best response |
|---|---|---|
| Eye opening (max 4) | 4 / 3 / 2 / 1 | spontaneous / to voice / to pain / none |
| Verbal (max 5) | 5 / 4 / 3 / 2 / 1 | oriented / confused / inappropriate words / incomprehensible sounds / none |
| Motor (max 6) | 6 / 5 / 4 / 3 / 2 / 1 | obeys / localises / withdraws / abnormal flexion / extension / none |
- Total GCS: max 15, min 3; mild 13-15, moderate 9-12, severe ≤8 (intubate).
- Pupils: unequal/fixed-dilated → herniation, usually side of the clot.
- Cushing reflex (raised ICP): HYPERtension + BRADYcardia + irregular respiration.
- Imaging: NCCT head is first-line.