Page 10 of 20
SU17.7 | Soft Tissue Injury Assessment and Management — SDL Guide
Learning Objectives
- Describe and classify soft tissue injuries — closed and open wounds — by mechanism and clinical features (SU17.7).
- Assess a soft tissue wound, including the structures deep to it, and choose appropriate investigations (SU17.7).
- Discuss the principles of management of soft tissue injuries, including wound closure, tetanus prophylaxis and antibiotics (SU17.7).
INSTRUCTIONS
Soft tissue injuries — from a simple graze to a limb-threatening degloving — are the commonest wounds a doctor will ever treat, and they look deceptively simple. The danger is rarely the skin defect you can see; it is the artery, nerve or tendon torn beneath it, the dirt ground into the tissue, and the risk of tetanus from an apparently trivial puncture. Good wound care is a disciplined routine: classify the injury, examine what lies deep to it, clean and close it correctly, and never forget tetanus. This module gives you that routine so that you can manage the common wound safely and recognise the one that hides a serious injury.
References
- Bailey & Love's Short Practice of Surgery, Wounds, Tissue Repair and Scars (textbook)
- SRB's Manual of Surgery, Wounds and Wound Healing (textbook)
- Sabiston Textbook of Surgery, Wound Healing and Soft Tissue Injury (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A farmer comes to the clinic having cut his forearm on a metal blade in his field. The wound is not large, and he is mainly worried about the bleeding, which has nearly stopped. It would be the easiest thing in the world to clean it, put in a few stitches, and send him home. But pause: the cut lies over the path of the tendons and nerves that move and feel his hand — has he lost the ability to bend a finger or feel its tip? The blade came from soil — is the wound now seeded with the dirt and devitalised tissue in which tetanus thrives, and when was he last immunised? A wound that looks trivial can hide a divided tendon, a transected nerve, or a lethal infection days away. The skill of soft-tissue injury care is learning to look past the obvious skin defect to the structures and the contamination beneath it.
WHY THIS MATTERS
Soft tissue injuries are everywhere in clinical practice — road traffic crashes, falls, assaults, occupational and household accidents, animal and human bites — and almost every one of them is first managed by a general doctor in casualty or a clinic, not a specialist. Managing them well prevents three avoidable disasters: a missed injury to a deep structure (a divided tendon or nerve that leaves a useless hand), a wound infection from inadequate cleaning or wrong closure, and tetanus from forgotten prophylaxis. Equally, knowing how to classify wounds matters medico-legally, because the type of wound (an incised wound versus a laceration, for example) carries legal weight in assessing how an injury was caused. These are core, examinable competencies for every graduate: you must be able to assess any wound systematically, decide how and when to close it, and give correct tetanus and antibiotic cover. Done properly, simple wound care delivers excellent outcomes; done carelessly, it causes lasting harm.
RECALL
Recall the foundations from earlier learning. From AN and your wound-healing studies: the skin has an outer epidermis, a dermis carrying vessels and nerves, and a subcutaneous layer, beneath which lie muscle, tendon, nerve and vessel — so the depth of a wound determines which of these is at risk. Recall the phases of wound healing — haemostasis, inflammation, proliferation (granulation and epithelialisation) and remodelling — because clean, well-apposed wounds heal by primary intention quickly, whereas contaminated or gaping wounds must heal by secondary intention with granulation tissue. From MI, recall that tetanus is caused by the exotoxin of Clostridium tetani, an anaerobe whose spores live in soil and faeces and germinate in devitalised, poorly oxygenated, contaminated wounds — which is exactly why wound contamination and immunisation status are central to soft-tissue care. Hold on to these, because assessment and management are built directly on them.
The Patient with a Wound
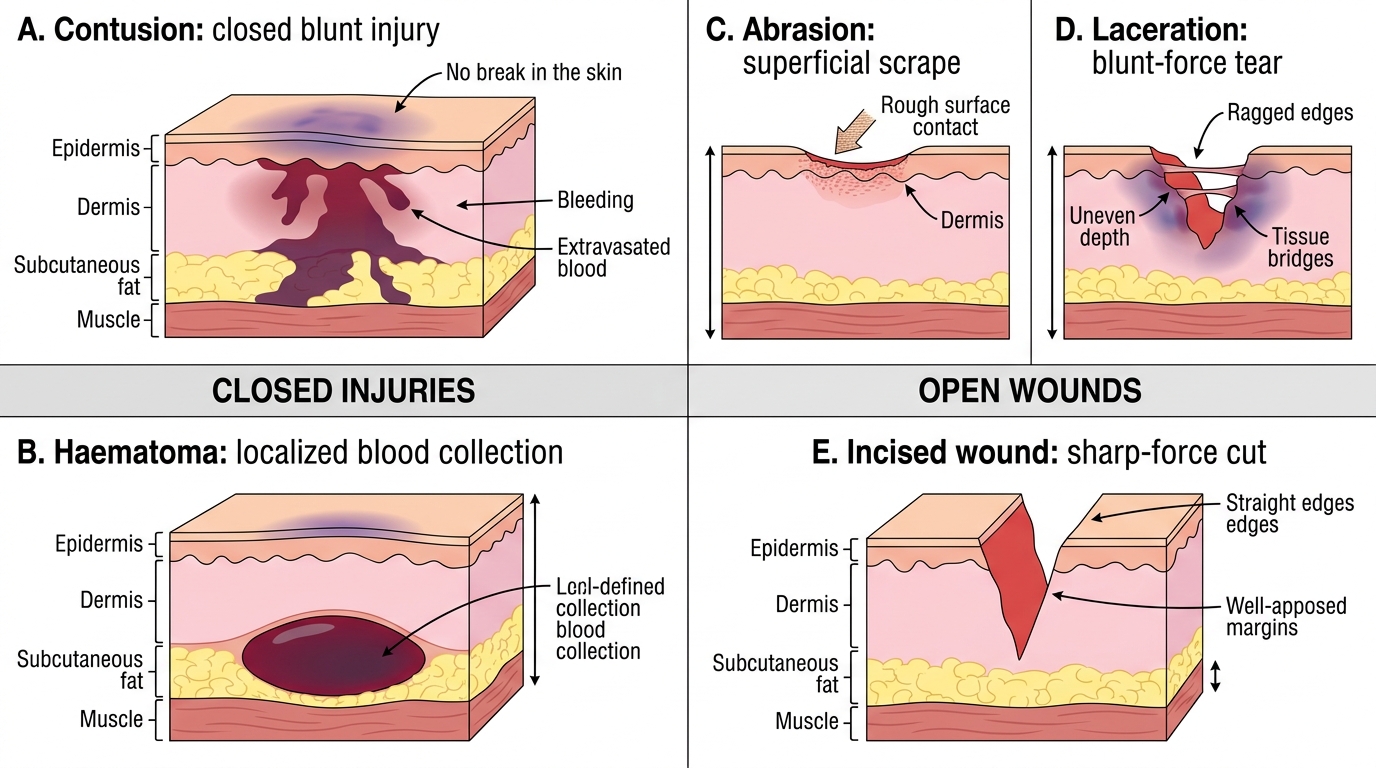
A soft tissue injury is any injury to the skin, subcutaneous tissue, muscle, tendon, ligament, nerve or blood vessel without (or before considering) a break in the bone, and its presentation spans an enormous range. At the trivial end is a closed injury such as a contusion (bruise) — bleeding into intact tissue from blunt force — or a sprain of a ligament; at the severe end is an open wound such as a degloving injury in which skin and subcutaneous tissue are sheared off the underlying fascia, or a contaminated crush with dead muscle. Between these lie the everyday grazes, cuts and punctures that fill any casualty department. The clinician's task is to read each wound on two levels at once: the visible damage (its size, depth, edges, contamination and bleeding) and the hidden damage to the structures that run beneath it. This second level is what makes soft-tissue care more than first aid — a small cut over a flexor tendon, a wrist, or the course of a major nerve or artery can carry a functionally devastating deep injury that is invisible on the surface. The presentation therefore guides the assessment: where the wound is, what caused it, how dirty it is, and what important structures lie deep to it all determine how serious it really is. Recognising that the wound you can see is only part of the injury is the first step to managing it safely.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
Spectrum of Soft Tissue Injuries
Types of Soft Tissue Injury and Their Basis
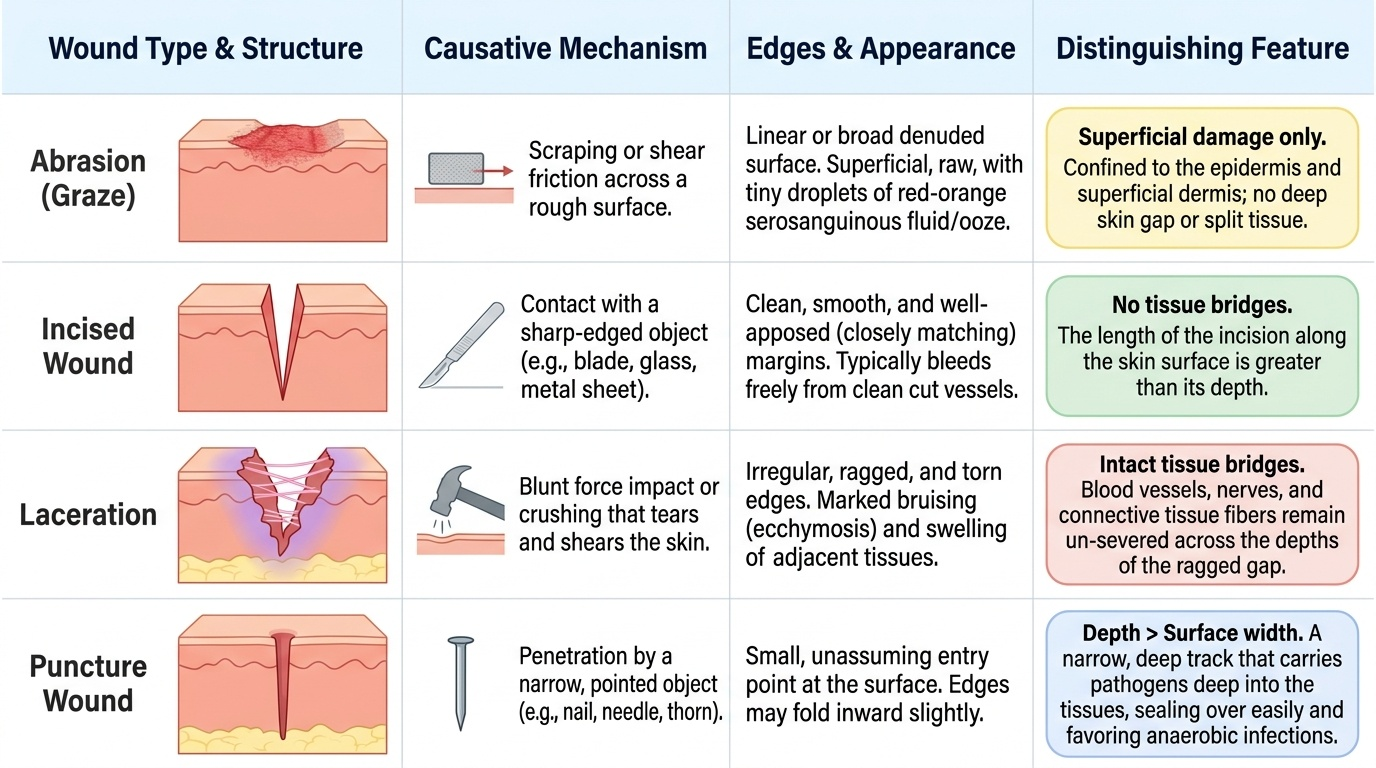
Soft tissue injuries are classified by whether the skin is broken and by the mechanism that caused them, and getting the classification right guides both treatment and, often, the medico-legal interpretation of how the injury happened. Closed injuries leave the skin intact: a contusion (bruise) is haemorrhage into the tissues from blunt force; a haematoma is a localised collection of blood; a sprain is the stretching or tearing of a ligament and a strain of a muscle or its tendon; and a crush injury involves prolonged compression that can devitalise muscle. Open wounds breach the skin and are distinguished by their mechanism and the appearance of their edges. An abrasion (graze) is the most superficial, involving only the epidermis and superficial dermis as the skin is scraped across a rough surface. An incised wound is a clean-edged cut produced by a sharp object such as a blade or glass, with smooth, well-apposed margins and no tissue bridges. A laceration is produced by blunt force that tears the skin, giving irregular, ragged edges, often with bruising and intact tissue bridges across the wound. A puncture (penetrating) wound is deep and narrow from a pointed object, dangerous because it carries contamination deep and seals over, favouring anaerobic infection. An avulsion tears a flap of tissue partly or completely free, and a degloving injury strips skin and subcutis off the underlying fascia. A bite wound (animal or human) combines a puncture and crush with heavy bacterial contamination. These distinctions are not academic: a clean incised wound may be closed primarily, whereas a contaminated laceration, puncture or bite needs careful cleaning, often delayed closure, and tetanus cover.
Provided image
| Wound type | Mechanism | Edges/appearance | Distinguishing feature |
|---|---|---|---|
| Abrasion (graze) | Scraping across a rough surface | Superficial, raw | Epidermis/superficial dermis only; no deep gap |
| Incised wound | Sharp object (blade, glass) | Clean, smooth, well-apposed | No tissue bridges; length > depth |
| Laceration | Blunt force tearing skin | Irregular, ragged, bruised | Tissue bridges present |
| Puncture/penetrating | Pointed object | Small entry, deep track | Carries contamination deep; anaerobic risk |
SELF-CHECK
A wound with clean, smooth, well-apposed edges and no tissue bridges, caused by a sharp blade, is best classified as which type?
A. Laceration
B. Abrasion
C. Incised wound
D. Contusion
Reveal Answer
Answer: C. Incised wound
An incised wound is produced by a sharp object and has clean, smooth, well-apposed margins with no tissue bridges. A laceration results from blunt force tearing the skin, giving irregular, ragged edges with intact tissue bridges; an abrasion is a superficial graze; a contusion is a closed bruise.
Assessing the Wound and Choosing Investigations
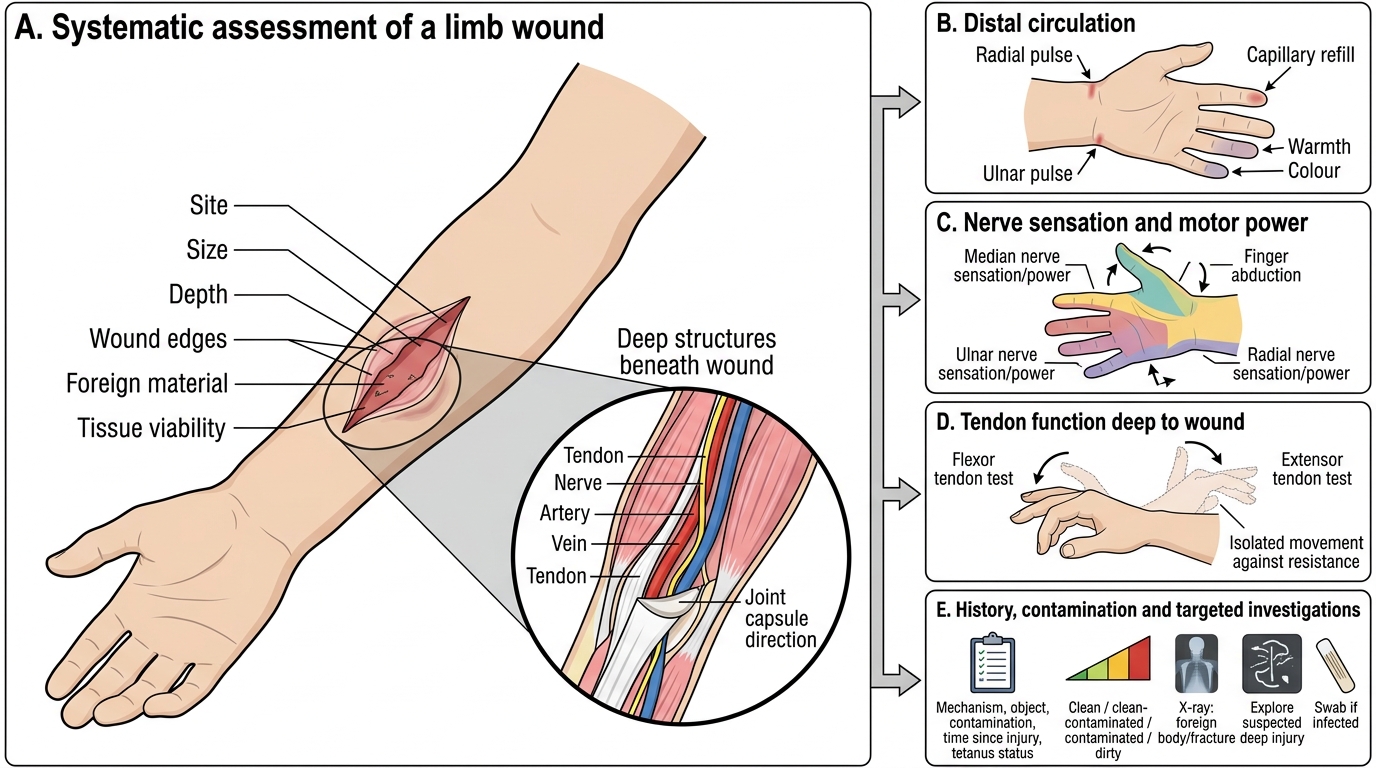
Assessment of a soft-tissue injury is a deliberate routine that examines both the wound and the structures deep to it, because the most important findings are often not in the skin defect itself. Begin with the history: the mechanism and the object (sharp, blunt, crush, bite), the degree of contamination (soil, faeces, saliva, water), the time since injury, and the patient's tetanus immunisation status — all of which shape management. Then examine the wound for its site, size, depth, edges, foreign material and the viability of its tissues, and control any bleeding for a clear look. Critically, assess the structures distal to and deep to the wound: check the circulation (distal pulses, colour, capillary refill — a divided artery threatens the limb), the nerves (sensation and motor power in the territory of nerves crossing the wound), and the tendons (test the specific movement each tendon produces, since a partially divided tendon can still move passively yet fail under load). A wound over a joint should also be assessed for joint penetration. Classify the wound's contamination (clean, clean-contaminated, contaminated or dirty), as this drives the closure decision and tetanus risk. Investigations are targeted, not routine: a plain X-ray is the key test where a radio-opaque foreign body (glass, metal) or an underlying fracture is suspected; formal wound exploration under anaesthesia is used when a deep structure injury is likely or the wound base cannot be seen; and swabs are taken from clearly infected wounds. A careful structured assessment is what separates a wound that is safely closed in casualty from one that needs theatre and a specialist.
Systematic Assessment of a Limb Wound
- History: mechanism, object, contamination, time since injury, tetanus status.
- Wound: site, size, depth, edges, foreign material, tissue viability.
- Deep structures (essential): distal circulation, nerve sensation/power, tendon function; joint penetration.
- Contamination class: clean / clean-contaminated / contaminated / dirty → guides closure and tetanus.
- Investigations (targeted): X-ray for foreign body/fracture; exploration for suspected deep injury; swab if infected.