Page 5 of 14
SU18.2 | Skin Tumors — SDL Guide (Part 2)
Differentiating the Tumors and Their Management
Management flows directly from differentiating the lesions, and the unifying surgical principle is complete excision with an adequate, histologically clear margin, the margin widening with the aggressiveness of the tumour. Benign lesions need treatment only for symptoms, diagnostic doubt or cosmesis: a lipoma is enucleated, a sebaceous cyst is excised completely (including its wall and punctum, to prevent recurrence), and a stable naevus is simply observed or excised if it changes or for cosmetic reasons. A basal cell carcinoma is treated by complete surgical excision with a margin of a few millimetres (Mohs micrographic surgery for ill-defined or recurrent facial lesions); because it rarely metastasises, nodal surgery is not needed, and radiotherapy is an alternative where surgery is difficult. A squamous cell carcinoma is excised with a wider margin and, because it can spread to nodes, the regional nodes are assessed and a block dissection performed if they are involved; a Marjolin's ulcer is managed as an aggressive SCC. Malignant melanoma is managed in two steps: the diagnostic excision biopsy establishes the Breslow thickness, then a wide local excision is performed whose margin is determined by that thickness (thicker tumours warrant wider margins). For intermediate and thick melanomas, sentinel lymph node biopsy is used to stage the regional nodes, a confirmed positive node leads to further nodal treatment, and advanced disease is increasingly treated with systemic immunotherapy and targeted therapy in addition to surgery.
Provided image
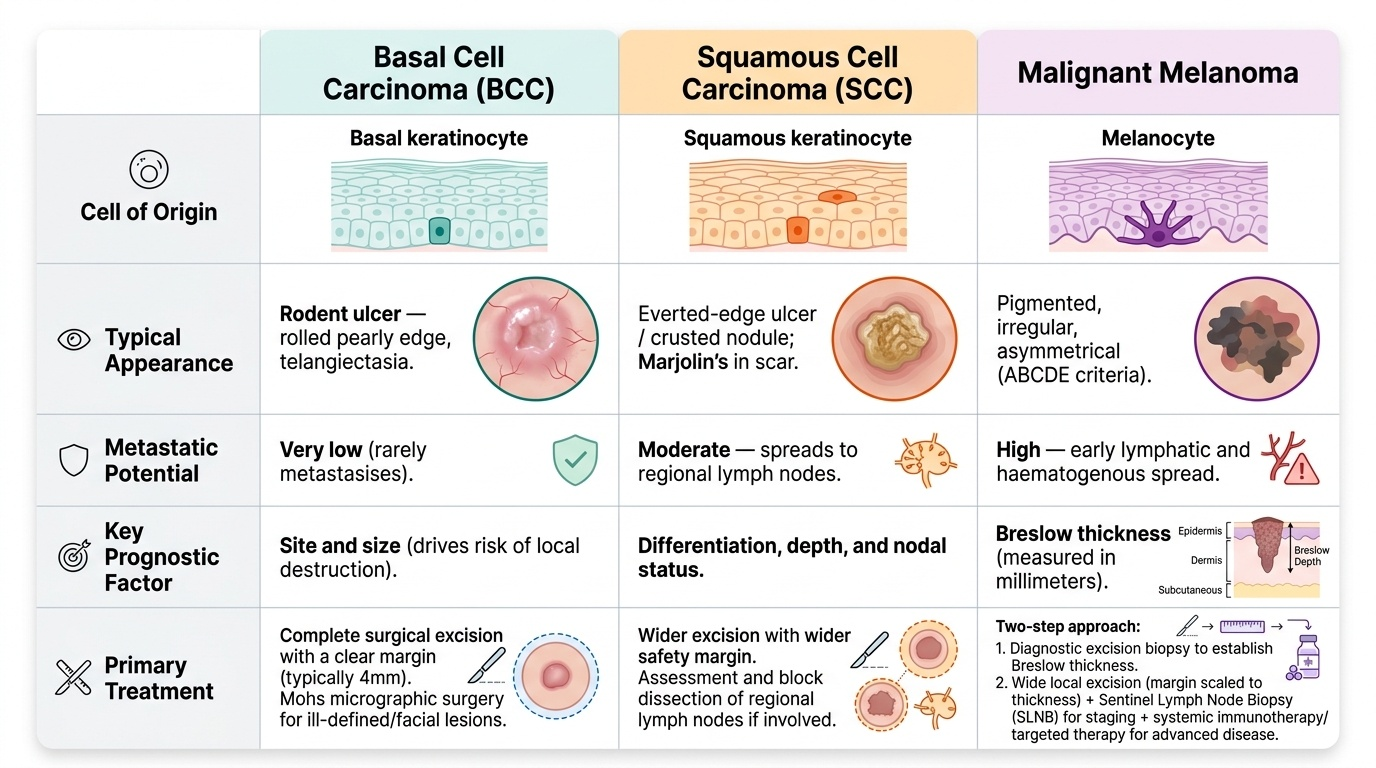
| Tumour | Cell of origin | Typical appearance | Metastatic potential | Key prognostic factor | Primary treatment |
|---|---|---|---|---|---|
| Basal cell carcinoma | Basal keratinocyte | Rodent ulcer — rolled pearly edge, telangiectasia | Very low (rarely metastasises) | Site and size (local destruction) | Complete excision with clear margin |
| Squamous cell carcinoma | Squamous keratinocyte | Everted-edge ulcer/crusted nodule; Marjolin's in scar | Moderate — to regional nodes | Differentiation, depth, node status | Wider excision ± nodal dissection |
| Malignant melanoma | Melanocyte | Pigmented, irregular (ABCDE) | High — lymphatic + haematogenous | Breslow thickness | Excision biopsy → wide local excision ± sentinel node biopsy |
CLINICAL PEARL
Two distinctions earn most of the marks and protect most patients. First, a basal cell carcinoma rarely metastasises and is dangerous by local erosion, whereas a squamous cell carcinoma can spread to the lymph nodes — so always palpate the draining nodes in an SCC and in any Marjolin's ulcer. Second, when you suspect a melanoma, perform a complete excision biopsy, not a shave or partial biopsy: only a full-thickness specimen lets the pathologist measure the Breslow thickness, the single most important prognostic factor, on which both the prognosis you give and the width of the definitive excision depend.
Check Your Understanding
Bring the threads together by reasoning back through the four patients in the hook. The young woman's soft, mobile, long-standing lump with a slip sign is a lipoma — benign, needing only reassurance or enucleation if symptomatic. The farmer's slowly enlarging, non-healing ulcer beside the nose with a raised, rolled, pearly edge is a basal cell carcinoma (rodent ulcer) — locally destructive but almost never metastasising, treated by complete excision. The heaped-up ulcer growing within the man's old burn scar is a Marjolin's ulcer, a squamous cell carcinoma — which can spread to nodes, so the draining nodes must be examined and the lesion widely excised. The teacher's mole that has darkened, grown and become irregular fits the ABCDE rule and is a suspected malignant melanoma — needing excision biopsy to measure the Breslow thickness that will determine her prognosis and definitive surgery. Use these to self-test the competency. First, can you place any skin lesion into the benign / premalignant / malignant classification? Second, can you differentiate BCC, SCC and melanoma by appearance, metastatic potential and key prognostic factor? Third, can you state the right biopsy and the principle of margin-based excision for each? The questions that follow check exactly these links.
SELF-CHECK
Which single factor is the most important determinant of prognosis in malignant melanoma?
A. The diameter of the lesion in centimetres
B. The colour of the lesion
C. The Breslow thickness (vertical tumour depth in millimetres)
D. The patient's age at diagnosis
Reveal Answer
Answer: C. The Breslow thickness (vertical tumour depth in millimetres)
The Breslow thickness — the vertical depth of tumour invasion measured in millimetres on histology — is the single most important prognostic factor in melanoma and also guides the width of the definitive wide local excision. This is why a suspected melanoma must be removed by complete excision biopsy rather than a shave or partial biopsy, which would prevent accurate measurement of the depth.