Page 8 of 14
SU21.1-2 | Disorders of Salivary Glands — SDL Guide (Part 2)
Principles of Treatment
Treatment of salivary gland disorders is determined by which of the three pathological groups the disease belongs to, and the unifying surgical principle for the parotid is the preservation of the facial nerve. For acute sialadenitis, treatment is initially conservative and medical: in acute bacterial parotitis, rehydration, attention to oral hygiene, sialogogues (agents such as citrus or chewing that stimulate salivary flow), warm compresses, gland massage and antibiotics usually resolve the infection, and the key preventive measure is maintaining hydration and oral care in vulnerable post-operative and debilitated patients; an abscess requires drainage, and recurrent chronic sialadenitis may eventually need gland excision. Viral parotitis (mumps) is managed supportively. For obstructive sialolithiasis, treatment depends on the site of the stone: a stone in the distal duct near its orifice can often be removed by simple transoral incision over the duct (sialolithotomy) or retrieved endoscopically by sialendoscopy, whereas stones in the hilum or within the substance of the submandibular gland, or a gland that has been repeatedly damaged by recurrent obstruction and infection, are best treated by excision of the submandibular gland. For neoplasms, the principle is adequate excision that removes the tumour with a cuff of normal tissue while preserving the facial nerve, never simple enucleation. The standard operation for a benign superficial-lobe parotid tumour, including the common pleomorphic adenoma, is a superficial parotidectomy with facial nerve preservation — enucleation is condemned because the pleomorphic adenoma's pseudopodia through its false capsule lead to recurrence. Deep-lobe tumours require total parotidectomy with nerve preservation. For a malignant parotid tumour, treatment is more radical — total parotidectomy, with sacrifice of the facial nerve only if it is directly involved by tumour (with nerve grafting where possible), neck dissection for nodal disease, and adjuvant radiotherapy for high-grade or advanced tumours. A submandibular tumour is treated by excision of the gland (wide local excision for malignancy). Whatever the operation, the surgeon must counsel the patient about the complications particular to salivary surgery: facial nerve injury (temporary or permanent), Frey's syndrome (gustatory sweating from aberrant reinnervation after parotidectomy), salivary fistula and, in submandibular surgery, injury to the marginal mandibular, lingual and hypoglossal nerves.
- Sialadenitis: conservative — rehydration, oral hygiene, sialogogues, warm compresses, antibiotics; drain an abscess; excise a chronically damaged gland.
- Sialolithiasis: distal duct stone → transoral sialolithotomy or sialendoscopy; hilar/intraglandular stone or damaged gland → submandibular gland excision.
- Benign parotid tumour (e.g. pleomorphic adenoma): superficial parotidectomy with facial nerve preservation — NEVER enucleation.
- Malignant parotid tumour: total parotidectomy, sacrifice facial nerve only if involved (graft if possible), neck dissection for nodes, adjuvant radiotherapy.
- Complications to counsel for: facial nerve injury, Frey's syndrome, salivary fistula; lingual/hypoglossal/marginal mandibular nerve injury in submandibular surgery.
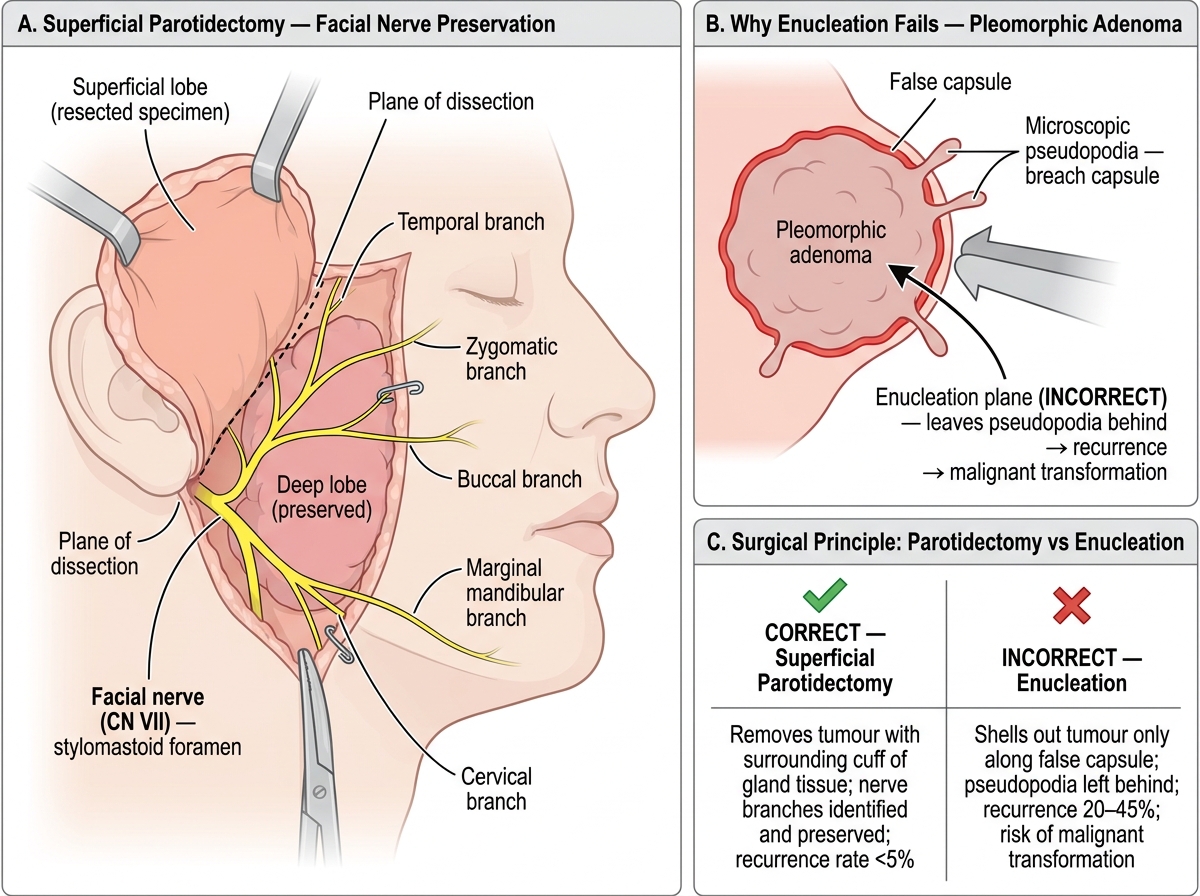
Superficial Parotidectomy: Facial Nerve Preservation and the Case Against Enucleation
CLINICAL PEARL
Two rules carry most of salivary surgery. First, a pleomorphic adenoma is NEVER enucleated — its microscopic pseudopodia push through a false capsule, so shelling it out leaves tumour behind and it recurs (and may turn malignant); the correct operation is a superficial parotidectomy with facial nerve preservation. Second, a facial nerve palsy in a patient with a parotid mass is a malignant tumour until proven otherwise — benign tumours, however large, characteristically spare the nerve, so a new facial weakness is a red flag, not a coincidence.
Check Your Understanding
Bring the threads together by returning to the three patients in the hook. The 45-year-old woman with a painless, rubbery, slowly growing parotid lump and an intact facial nerve has the classic picture of a benign pleomorphic adenoma; she should have FNAC and ultrasound/MRI, and the correct treatment is a superficial parotidectomy with facial nerve preservation, not enucleation. The 30-year-old man whose submandibular gland swells and aches at mealtimes has sialolithiasis: a plain radiograph or ultrasound will look for the radio-opaque submandibular stone, and treatment is transoral removal or sialendoscopy for a distal stone, or gland excision for a hilar/intraglandular stone or a damaged gland. The dehydrated post-operative man with a hot, tender, diffusely swollen parotid has acute bacterial sialadenitis, treated by rehydration, oral hygiene, sialogogues and antibiotics, with drainage if an abscess forms. Use these to self-test the two competencies this module covers. First, can you describe the surgical anatomy (especially the facial nerve dividing the parotid into superficial and deep lobes, and Wharton's duct's uphill course explaining submandibular stones) and the pathology and presentation of inflammatory, obstructive and neoplastic disorders? Second, can you enumerate the appropriate investigations (FNAC, ultrasound, MRI/CT, sialography/sialendoscopy, plain radiograph for stones — and why open biopsy of a parotid lump is avoided) and describe the principles of treatment, above all facial-nerve-preserving surgery and never enucleating a pleomorphic adenoma? The questions that follow check exactly these links.
SELF-CHECK
A 45-year-old woman has a painless, mobile, rubbery 2 cm lump in the superficial part of the parotid with a normal facial nerve; FNAC suggests a pleomorphic adenoma. What is the correct surgical treatment?
A. Enucleation of the lump alone
B. Superficial parotidectomy with preservation of the facial nerve
C. Radiotherapy without surgery
D. Total parotidectomy with deliberate sacrifice of the facial nerve
Reveal Answer
Answer: B. Superficial parotidectomy with preservation of the facial nerve
A pleomorphic adenoma must NOT be enucleated, because its microscopic pseudopodia extend through a false capsule, so enucleation leaves tumour behind and causes recurrence (with a risk of malignant change). The correct operation is a superficial parotidectomy with identification and preservation of the facial nerve. Sacrificing the nerve is reserved for malignant tumours that directly involve it.