Page 4 of 14
SU20.1-2 | Oropharyngeal Cancer — SDL Guide
Learning Objectives
- Describe the aetiopathogenesis of oral cancer and the symptoms and signs of oropharyngeal cancer (SU20.1).
- Enumerate the appropriate investigations and discuss the principles of treatment of oropharyngeal cancer (SU20.2).
INSTRUCTIONS
Oral and oropharyngeal cancer is one of the most important cancers in India, driven overwhelmingly by tobacco and areca-nut use, and it is one of the few cancers a clinician can see and feel directly at the bedside. The central message of this module is that this is a largely preventable, often visible disease that is curable when caught early and devastating when caught late — and that the bridge between the two is recognising premalignant lesions and the early signs. We connect the carcinogenesis and risk factors to the symptoms and signs, the triple-assessment work-up and TNM staging, and the stage-directed principles of treatment.
References
- Bailey & Love's Short Practice of Surgery, The Mouth and Tongue / Oral and Oropharyngeal Cancer (textbook)
- SRB's Manual of Surgery, Oral Cavity, Lip and Tongue (textbook)
- Sabiston Textbook of Surgery, Head and Neck — Oral Cavity and Oropharynx (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 52-year-old man who has chewed tobacco and areca nut for thirty years comes to clinic because of an ulcer on the side of his tongue that has not healed for two months and now hurts when he eats. He has lost a little weight, his mouth feels stiff, and over the last week he has noticed a hard lump in his neck. He had ignored a white patch in the same part of his mouth for years. Sitting across from him is everything a clinician fears about this disease and everything that should have prevented it: a visible, palpable cancer arising in a mouth that gave warning signs — a premalignant white patch and a non-healing ulcer — over which a simple examination, performed earlier, could have changed the outcome entirely. Oral and oropharyngeal cancer is a disease you can see and feel, and the difference between an early curable lesion and a late incurable one is very often the difference between looking and not looking.
WHY THIS MATTERS
Oral and oropharyngeal cancer carries enormous weight in Indian surgical practice: India has among the highest incidence rates in the world, almost entirely because of the chewing of tobacco and areca (betel) nut, making this a leading cancer in men and a major public-health problem. It matters clinically for three reasons. First, it is largely preventable — stopping tobacco and areca-nut use would remove most of the disease — so every clinical contact is a chance to counsel. Second, it is visible and palpable, so it is one of the few internal cancers that an alert generalist can detect early simply by examining the mouth, which is why recognising premalignant lesions and a non-healing ulcer is a core skill. Third, the gulf between early and late disease is stark: an early lesion is highly curable with single-modality treatment and good function, whereas advanced disease needs disfiguring surgery and chemoradiation with poor outcomes. For a final-year student, knowing the risk factors, the warning lesions, the triple-assessment work-up and the principles of stage-directed treatment is directly life-saving knowledge.
RECALL
Recall some foundations before we build on them. From anatomy: the oral cavity extends from the lips to the junction of the hard and soft palate and the line of the circumvallate papillae, and includes the lips, buccal mucosa, alveolus and gingiva, the anterior two-thirds of the tongue, the floor of the mouth and the hard palate; the oropharynx lies behind it and includes the base of the tongue, the tonsils, the soft palate and the posterior pharyngeal wall. From oncology, recall that the mucosal lining here is stratified squamous epithelium, which is why the overwhelming majority of cancers at these sites are squamous cell carcinomas. Recall, too, the rich lymphatic drainage of the mouth and oropharynx to the cervical lymph nodes (levels I-V of the neck), which explains why a neck mass is so often the presenting feature and why the neck must be assessed and frequently treated. Finally, recall the principle of TNM staging — describing the primary Tumour, the regional Nodes and distant Metastases — which is the common language used to stage and direct treatment for almost all solid cancers, including this one.
The Patient with a Mouth or Throat Lesion
Oral and oropharyngeal cancer announces itself in ways that are easy to recognise once you are looking for them, and the single most important clinical rule is that any oral ulcer that fails to heal within about three weeks must be regarded as cancer until proven otherwise. The classic presentation is a non-healing ulcer — typically with raised, rolled or everted edges, an indurated (hard) base and surrounding firmness — most often on the lateral border of the tongue, the floor of the mouth or the buccal mucosa. Cancer may also present as a persistent white or red patch (a leukoplakia or erythroplakia that has undergone malignant change), as a proliferative or exophytic growth, or as a fungating mass. As the disease advances, patients develop pain, which is often referred to the ear (otalgia) because the tongue and oropharynx share sensory innervation with the ear; difficulty and pain on swallowing (dysphagia and odynophagia), particularly with oropharyngeal lesions; difficulty in speaking and a change in voice; trismus (restricted mouth opening) from involvement of the muscles of mastication or from coexistent oral submucous fibrosis; bleeding from the mouth, foul breath (halitosis) and excessive salivation or drooling; and loosening of teeth where the alveolus is involved. A very common — and ominous — presentation is a hard, enlarged cervical lymph node, reflecting nodal metastasis, and the lump in the neck may be what finally brings the patient in. Constitutional features such as weight loss and anorexia point to advanced disease. On examination the lesion is inspected and, crucially, palpated bimanually to assess its extent, induration and fixity, the whole oral cavity and oropharynx are inspected (a lesion may be multifocal), and the neck is examined systematically for lymphadenopathy — because the state of the neck powerfully influences both staging and prognosis.
- Hallmark: non-healing ulcer (>3 weeks) with raised/everted edges and indurated base — cancer until proven otherwise.
- Other primary signs: persistent white/red patch, proliferative growth, fungating mass.
- Symptoms of progression: pain/referred otalgia, dysphagia/odynophagia, dysphonia, trismus, bleeding, halitosis, loose teeth.
- Spread: hard cervical lymph node (common presentation); weight loss = advanced disease.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
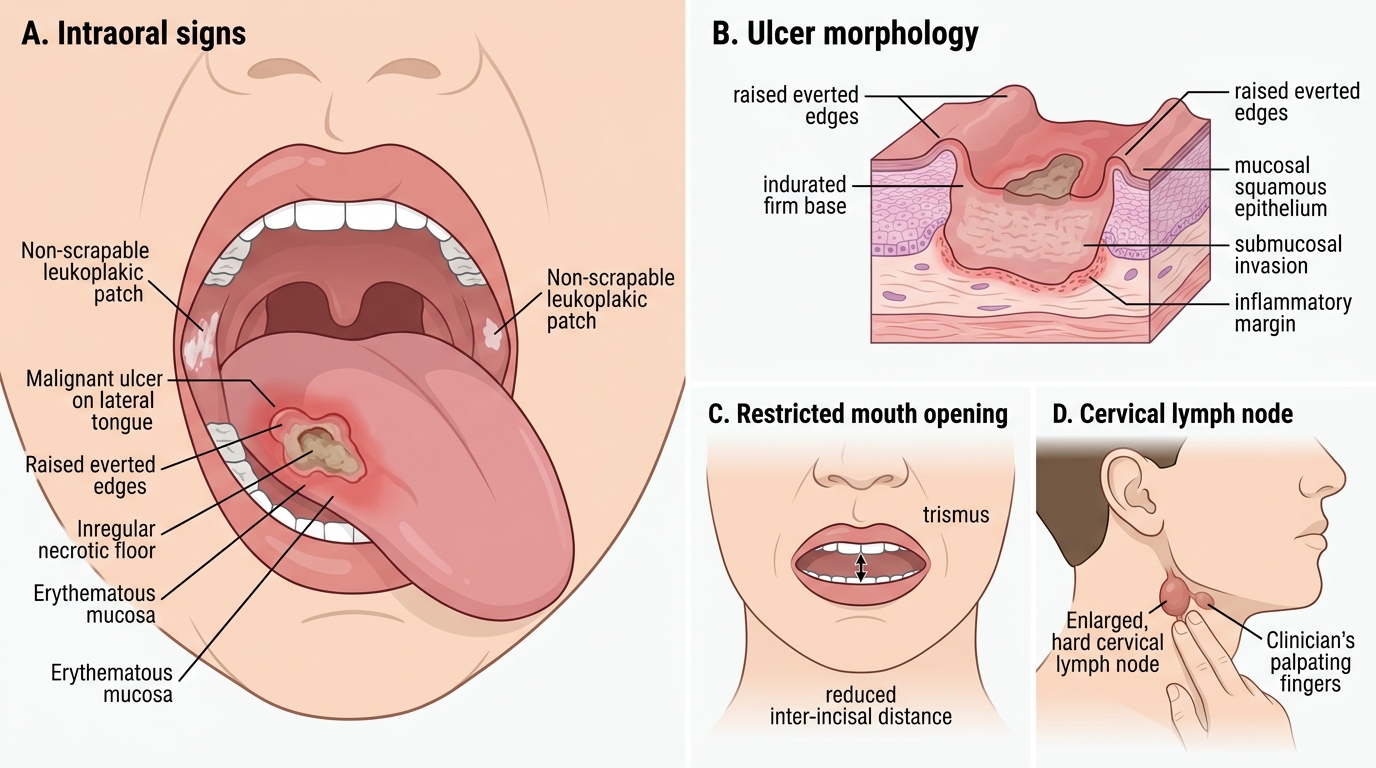
Clinical Signs of Oral and Oropharyngeal Cancer
Aetiopathogenesis and Premalignant Lesions
More than 90% of oral and oropharyngeal cancers are squamous cell carcinomas (SCC), arising from the mucosal squamous epithelium, and the aetiology is dominated by identifiable, modifiable carcinogens. The leading cause in India and much of South Asia is smokeless tobacco and areca (betel) nut chewing — the habit of holding a tobacco-areca quid against the buccal mucosa delivers carcinogens directly and for prolonged periods to the mucosa, which is why buccal and gingivobuccal cancers are so common here. Smoking tobacco and alcohol are independent risk factors that act synergistically (their combined effect is greater than the sum of each alone), and human papillomavirus (HPV), particularly HPV-16, is an increasingly important cause specifically of oropharyngeal SCC (base of tongue and tonsil); importantly, HPV-positive oropharyngeal cancer tends to occur in younger, non-smoking patients and carries a distinctly better prognosis than HPV-negative, tobacco-related disease. Other contributors include chronic irritation (sharp teeth, ill-fitting dentures), poor oral hygiene, sunlight exposure for lip cancer and nutritional deficiency. The crucial pathological concept is that most of these cancers develop through recognisable premalignant (potentially malignant) lesions, and identifying them is the chief opportunity for prevention and early cure. Leukoplakia is a white patch that cannot be wiped off and cannot be attributed to any other disease; it carries a definite but relatively low risk of malignant transformation. Erythroplakia is a red velvety patch and, although less common, carries a substantially higher risk of malignant change than leukoplakia, so a red patch is more sinister than a white one. Oral submucous fibrosis (OSMF) is a chronic, progressive, premalignant condition strongly linked to areca-nut chewing, characterised by mucosal fibrosis, blanching, burning and progressive trismus (inability to open the mouth). Any of these lesions that changes — thickening, ulceration, induration or bleeding — must be biopsied promptly. Once invasive, SCC spreads by local infiltration into adjacent muscle, bone and structures and by lymphatic spread to the cervical nodes (the dominant route), with blood-borne distant metastasis being relatively late.
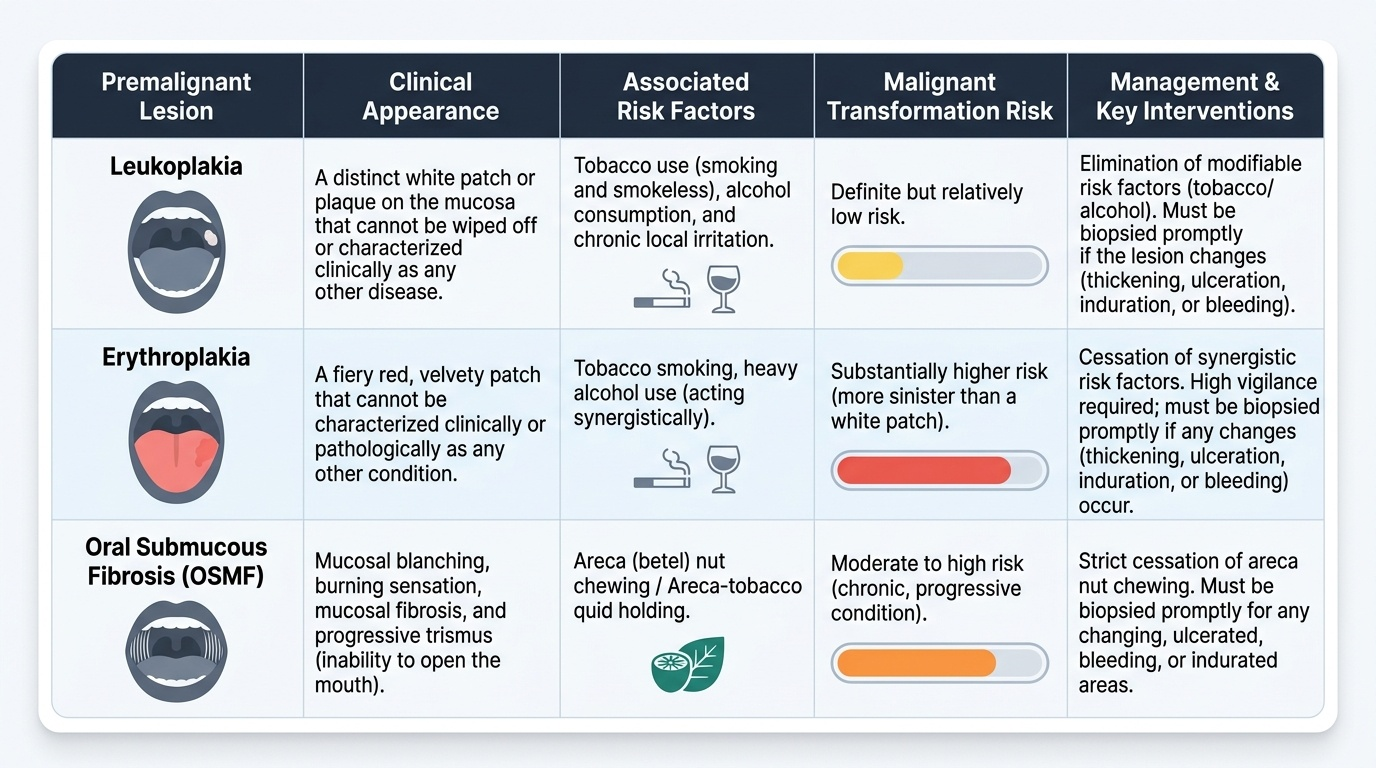
Provided image
- Histology: >90% squamous cell carcinoma.
- Risk factors: smokeless tobacco + areca/betel nut (dominant in India), smoking, alcohol (synergistic), HPV-16 (oropharynx; better prognosis), chronic irritation.
- Premalignant lesions: leukoplakia (white, lower risk), erythroplakia (red, higher risk), oral submucous fibrosis (areca-nut, fibrosis + trismus).
- Spread: local infiltration; lymphatic to cervical nodes (dominant); haematogenous (late).
SELF-CHECK
Which premalignant oral lesion carries the HIGHEST risk of malignant transformation and so is the most sinister to find on examination?
A. Leukoplakia (white patch)
B. Erythroplakia (red patch)
C. A traumatic ulcer from a sharp tooth
D. A simple mucous retention cyst
Reveal Answer
Answer: B. Erythroplakia (red patch)
Erythroplakia, the red velvety patch, carries a substantially higher risk of malignant transformation than leukoplakia (the white patch). A red patch in the mouth should therefore be regarded as more dangerous than a white one and biopsied promptly. Oral submucous fibrosis is also premalignant but is characterised by fibrosis and trismus rather than being the single highest-risk patch.
Investigations and Staging
The investigation of a suspected oral or oropharyngeal cancer follows the universal oncological principle of triple assessment — combining clinical examination, imaging and tissue diagnosis — supplemented by panendoscopy to exclude synchronous tumours, the whole purpose being to confirm the diagnosis and to stage the disease so that treatment can be planned. The first arm is clinical assessment: careful inspection and bimanual palpation of the lesion to map its size and extent, examination of the entire oral cavity and oropharynx for multifocal disease, and systematic examination of the neck for nodal metastases. The second arm is tissue diagnosis, which is mandatory before any treatment: an incisional biopsy of the lesion (taken from the edge, including some normal tissue) provides the histological confirmation of SCC and its grade, while fine-needle aspiration cytology (FNAC) is used to confirm a metastatic cervical node. The third arm is imaging to define local extent and spread: contrast-enhanced CT and/or MRI of the head and neck assesses the depth of invasion, bone involvement (mandible/maxilla) and the cervical nodes, a chest radiograph or CT screens for pulmonary metastasis and a second primary, and PET-CT is used in selected advanced cases to detect occult metastases and to evaluate the post-treatment neck. Because patients with these tobacco-related cancers are at high risk of a second primary tumour elsewhere in the upper aerodigestive tract, panendoscopy (examination of the oral cavity, pharynx, larynx and oesophagus under anaesthesia) is performed to exclude synchronous lesions and to assess the airway. All of this information is then assembled into a TNM stage, describing the size and local extent of the primary Tumour, the presence and extent of regional lymph Node involvement, and distant Metastasis. The TNM stage is the single most important determinant of treatment choice and prognosis, which is why no treatment decision is made until staging is complete.
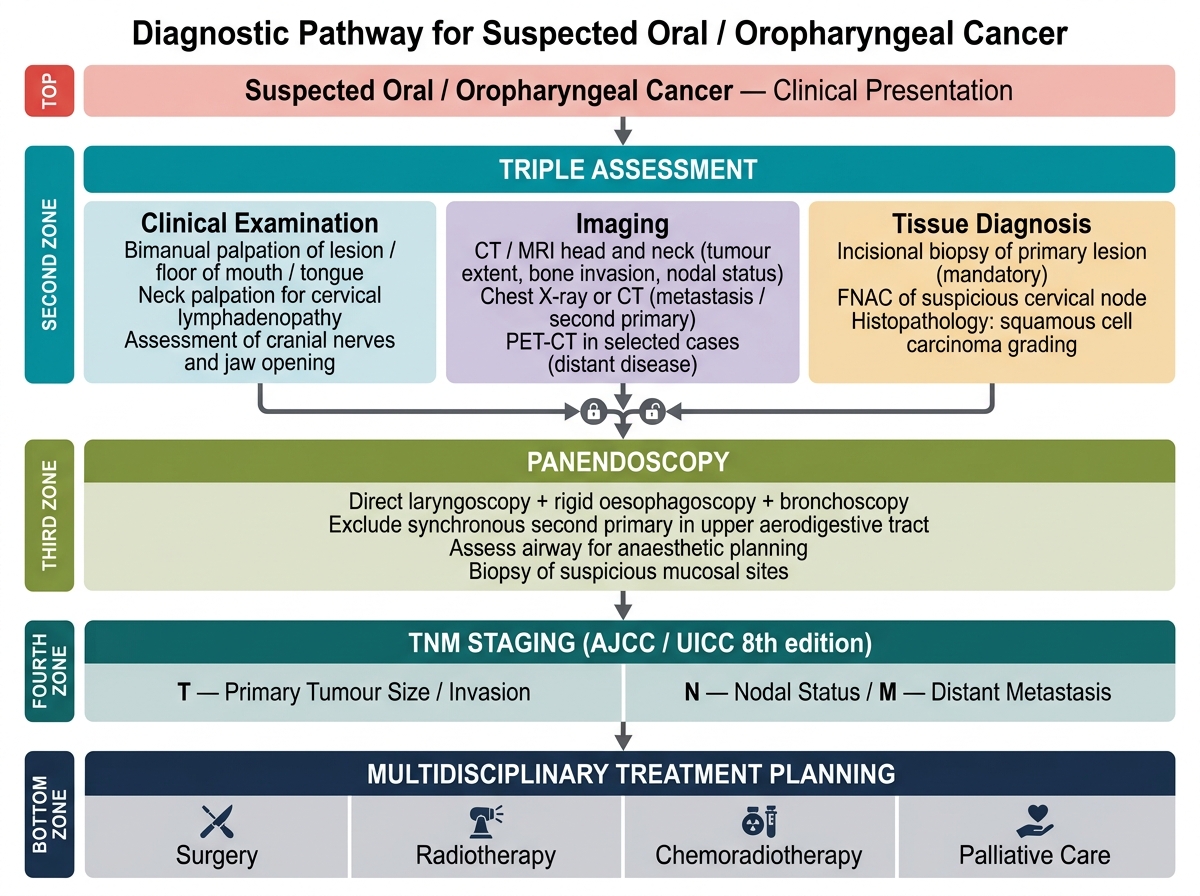
Diagnostic Pathway for Suspected Oral / Oropharyngeal Cancer
- Triple assessment: clinical examination (bimanual palpation + neck) + imaging + tissue diagnosis.
- Tissue: incisional biopsy of the lesion (mandatory); FNAC of a suspicious neck node.
- Imaging: CT/MRI head and neck (extent, bone, nodes); chest imaging (metastasis/second primary); PET-CT in selected cases.
- Panendoscopy: exclude synchronous second primary in the upper aerodigestive tract; assess airway.
- Output: TNM stage → governs treatment and prognosis.