Page 8 of 14
SU22.5-6 | Parathyroid Anatomy and Parathyroid Disorders — SDL Guide (Part 2)
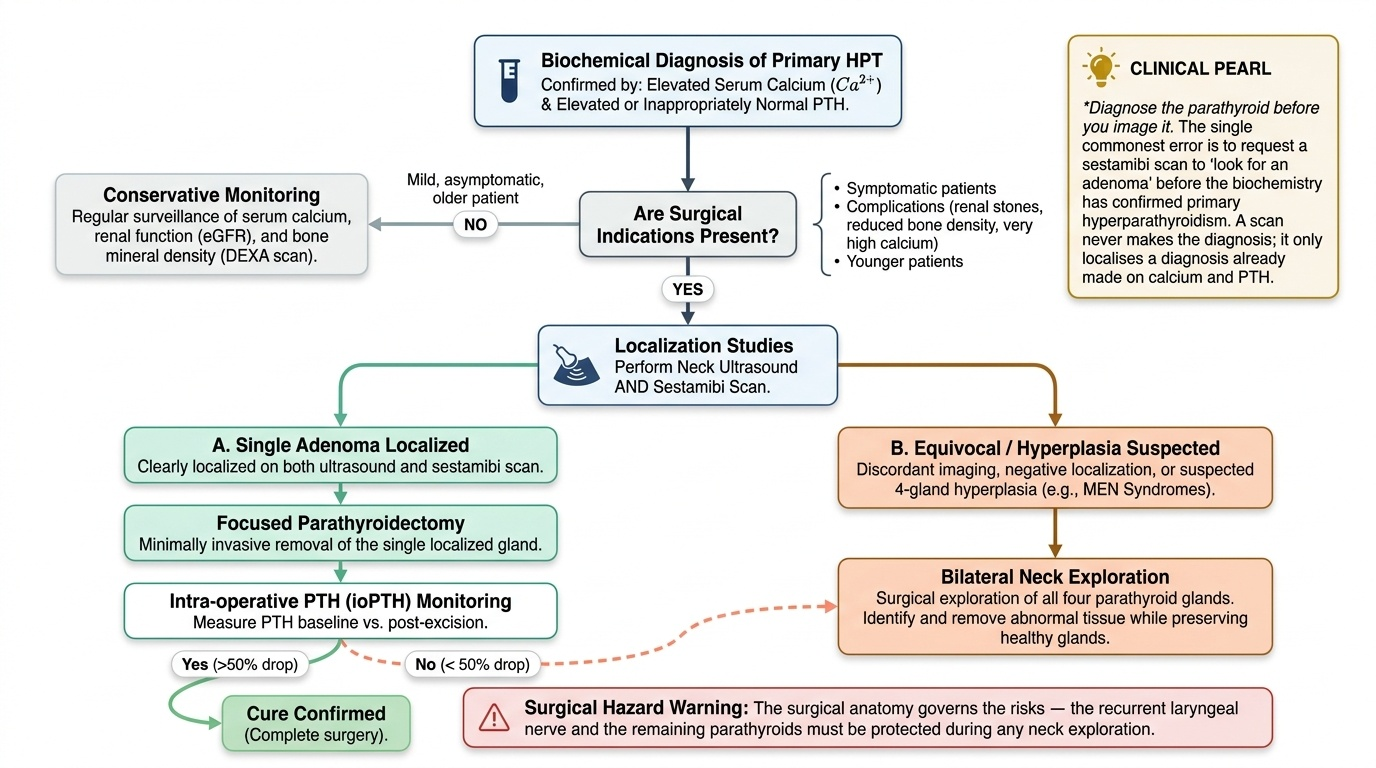
Principles of Management
Management is matched to the type of parathyroid disturbance. Primary hyperparathyroidism is a surgical disease: parathyroidectomy is curative, and symptomatic patients, those with complications (renal stones, reduced bone density, very high calcium) and younger patients should be offered surgery. When a single adenoma has been clearly localised on ultrasound and sestamibi, a focused (minimally invasive) parathyroidectomy removes just that gland, often guided by intra-operative PTH monitoring — a fall of more than 50% after excision confirms cure; if localisation is equivocal or four-gland hyperplasia is suspected (as in MEN syndromes), bilateral neck exploration is performed. Mild, asymptomatic disease in older patients may instead be monitored. Secondary hyperparathyroidism is primarily a medical problem managed by treating the underlying chronic kidney disease — phosphate binders, active vitamin D analogues and calcimimetics — with parathyroidectomy reserved for disease refractory to medical control. Hypoparathyroidism, most often a complication of thyroid or parathyroid surgery, is treated by correcting the hypocalcaemia: urgent intravenous calcium for symptomatic or severe cases, and longer-term oral calcium and active vitamin D. As always, the surgical anatomy governs the risks — the recurrent laryngeal nerve and the remaining parathyroids must be protected during any neck exploration.
Provided image
- Primary HPT: parathyroidectomy (focused if localised; bilateral exploration if not / hyperplasia); intra-operative PTH (>50% fall = cure); monitor mild asymptomatic disease.
- Secondary HPT: medical (treat CKD — phosphate binders, vitamin D analogues, calcimimetics); surgery if refractory.
- Hypoparathyroidism: IV calcium if severe/symptomatic; long-term oral calcium + active vitamin D.
CLINICAL PEARL
Diagnose the parathyroid before you image it. The single commonest error is to request a sestamibi scan to 'look for an adenoma' before the biochemistry has confirmed primary hyperparathyroidism — but a scan never makes the diagnosis, it only localises a diagnosis already made on calcium and PTH. Fix the order in your mind: high calcium with a non-suppressed PTH first, then ultrasound and sestamibi to find the gland, then surgery. And before calling any hypercalcaemia 'primary hyperparathyroidism', send a urinary calcium to exclude familial hypocalciuric hypercalcaemia, the benign mimic you must never operate on.
Check Your Understanding
Use these prompts to consolidate the two halves of this module — the applied anatomy of the glands and the clinical reasoning about calcium. Write a structured answer to each in your own words before checking it against the sections above, and pay particular attention to the biochemical patterns, because correctly reading the serum calcium against the PTH (and phosphate) is the single discrimination on which every parathyroid decision rests. Notice as you work through them that the same small glands explain two opposite clinical pictures: too much hormone drives the calcium up and gives the classic picture of stones, bones, groans and moans, while too little, most often after thyroid surgery, drops the calcium and produces tetany. Test yourself on the anatomy that makes these glands vulnerable during thyroidectomy, on separating primary, secondary and tertiary hyperparathyroidism by their biochemistry, and on the logical order of diagnosis, then localisation, then treatment, since reversing that order is the commonest practical error in managing these patients.
- Describe the number, usual position, embryological origin and blood supply of the parathyroid glands, and explain why they are at risk during thyroidectomy.
- Tabulate primary, secondary and tertiary hyperparathyroidism and hypoparathyroidism by serum calcium and PTH, and give a typical cause of each.
- List the clinical features of hypercalcaemia using the classic mnemonic, and the features of hypocalcaemia including the two eponymous signs.
- Outline the management of a patient with symptomatic primary hyperparathyroidism, from confirming the diagnosis through localisation to the choice of operation.
SELF-CHECK
After a total thyroidectomy a patient develops perioral tingling and a positive Trousseau's sign. What is the most likely cause?
A. Recurrent laryngeal nerve injury
B. Hypocalcaemia from injury to or removal of the parathyroid glands
C. Thyroid storm
D. Wound haematoma
Reveal Answer
Answer: B. Hypocalcaemia from injury to or removal of the parathyroid glands
Perioral paraesthesiae and a positive Trousseau's sign are features of hypocalcaemia. The parathyroid glands lie on the posterior thyroid and share its (inferior thyroid artery) blood supply, so they can be removed or devascularised during thyroidectomy, causing hypoparathyroidism and hypocalcaemia. This is treated with calcium and active vitamin D.