Page 2 of 14
SU22.1-3 | Thyroid Anatomy, Physiology and Swellings — SDL Guide (Part 2)
Differential Diagnosis and Surgical Management
The differential of a thyroid swelling runs from the entirely benign to the lethal, and management follows directly from where the work-up places the lump. Benign diffuse and colloid goitres that are euthyroid and asymptomatic can often simply be observed; surgery is reserved for pressure symptoms, cosmetic concern, suspicion of malignancy, or a toxic gland not controlled medically. When malignancy is the question, it is essential to know that thyroid cancers are distinct diseases, not one entity. Papillary carcinoma is the commonest, typically in younger patients, spreads chiefly via lymphatics to cervical nodes, and has an excellent prognosis. Follicular carcinoma spreads chiefly by the bloodstream to lung and bone and cannot be diagnosed by FNAC alone because the diagnosis rests on demonstrating capsular or vascular invasion on histology. Medullary carcinoma arises from the calcitonin-secreting parafollicular C cells, may be familial as part of MEN-2, and is screened with calcitonin. Anaplastic carcinoma is an undifferentiated, rapidly fatal tumour of the elderly. Surgical options range from a hemithyroidectomy (lobectomy) for an indeterminate or low-risk unilateral nodule to total thyroidectomy for confirmed cancer or bilateral disease, with central/lateral neck dissection where nodes are involved. Whatever the extent, the operation is defined by what is preserved: the recurrent and external laryngeal nerves and the parathyroid glands. The cardinal early complications to consent for and watch for are recurrent laryngeal nerve palsy (voice change), hypoparathyroidism with hypocalcaemia (perioral tingling, Chvostek and Trousseau signs, tetany), and reactionary haemorrhage causing airway compromise.
Provided image
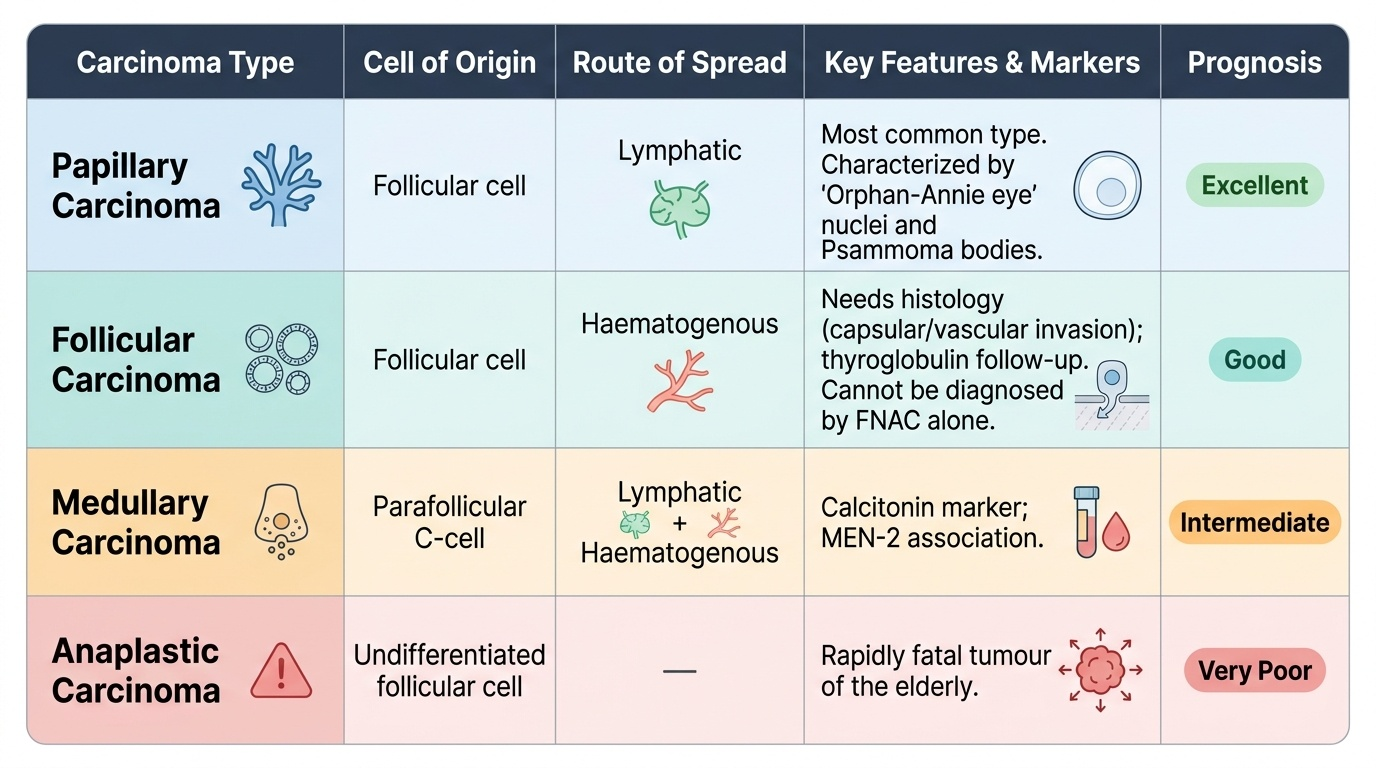
| Carcinoma | Cell of origin | Route of spread | Key feature/marker | Prognosis |
|---|---|---|---|---|
| Papillary | Follicular cell | Lymphatic | Commonest; psammoma bodies, 'Orphan-Annie' nuclei | Excellent |
| Follicular | Follicular cell | Haematogenous (lung/bone) | Needs histology (capsular/vascular invasion); thyroglobulin follow-up | Good |
| Medullary | Parafollicular C cell | Lymphatic + haematogenous | Calcitonin; MEN-2 association | Intermediate |
| Anaplastic | Undifferentiated follicular | Local + distant | Elderly, rapidly progressive, fixed mass | Very poor |
CLINICAL PEARL
A solitary thyroid nodule with a NORMAL or raised TSH should go to ultrasound and FNAC — do not be falsely reassured that 'thyroid function is normal'. Only a SUPPRESSED TSH justifies a radionuclide scan first to look for a benign autonomously functioning ('hot') nodule, because hot nodules are almost never malignant and are not usually aspirated. Skipping straight to FNAC in a suppressed-TSH nodule wastes a step; skipping FNAC in a normal-TSH nodule risks missing a cancer.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The young woman with a long-standing, painless, smoothly moving, euthyroid lump and no red flags sits at the benign end: a structured examination, a normal TSH, reassuring ultrasound and a benign FNAC (Bethesda II) would justify observation. The elderly man with a hard, fixed, rapidly growing mass and a hoarse voice sits at the malignant end: that voice change implies recurrent laryngeal nerve involvement and demands urgent ultrasound, FNAC and laryngoscopy, with anaplastic or advanced carcinoma high on the differential. Use these to self-test the three competencies this module covers. First, can you name the surgically critical anatomical relations — superior thyroid artery with external laryngeal nerve, inferior thyroid artery with recurrent laryngeal nerve, and the parathyroids — and the deficit each injury produces? Second, can you classify thyroid swellings and distinguish the four carcinoma types by cell of origin, spread and prognosis? Third, can you perform and document the examination and state the TSH → ultrasound → FNAC(Bethesda) work-up in the correct order? The questions that follow check exactly these links.
SELF-CHECK
Which thyroid carcinoma arises from the parafollicular C cells, secretes calcitonin, and may occur as part of MEN-2?
A. Papillary carcinoma
B. Follicular carcinoma
C. Medullary carcinoma
D. Anaplastic carcinoma
Reveal Answer
Answer: C. Medullary carcinoma
Medullary carcinoma originates from the calcitonin-secreting parafollicular C cells and is associated with MEN-2 (so a family history matters). Papillary and follicular carcinomas are follicular-cell-derived; anaplastic is an undifferentiated, rapidly fatal tumour of the elderly.