Page 1 of 17
SU23.1-2 | Adrenal Anatomy and Adrenal Disorders — SDL Guide
Learning Objectives
- Describe the applied surgical anatomy of the adrenal glands, including their retroperitoneal position, blood supply and the asymmetric venous drainage relevant to adrenalectomy (SU23.1).
- Relate the histological zones of the adrenal cortex and the medulla to the hormones they secrete and to the functional disorders produced by their excess (SU23.1, SU23.2).
- Describe the etiology, clinical features and principles of investigation and management of the major adrenal disorders — Cushing's syndrome, Conn's syndrome, phaeochromocytoma and the adrenal incidentaloma (SU23.2).
INSTRUCTIONS
The adrenal glands are small, deep and easily forgotten — until a patient presents with hypertension that will not yield to three drugs, a moon face and easy bruising, or terrifying paroxysms of headache, sweating and palpitations. Each of those stories points to a different hormone made in a different layer of the same gland, and the surgical task is the same throughout: prove which hormone is in excess, find where it is coming from, optimise the patient medically, and only then remove the gland safely. This module connects the surgical anatomy and the cortex-and-medulla physiology to a disciplined, hormone-first work-up and to the principles of adrenalectomy — including the one rule that can save a life in theatre: in phaeochromocytoma, alpha-blockade always comes before beta-blockade.
References
- Bailey & Love's Short Practice of Surgery, The Adrenal Glands and Other Abdominal Endocrine Disorders (textbook)
- SRB's Manual of Surgery, Adrenal Gland (textbook)
- Sabiston Textbook of Surgery, The Adrenal Gland (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 34-year-old woman has been referred with hypertension that three different drugs have failed to control, and a routine potassium has come back persistently low. In the next cubicle a 45-year-old man has gained weight only around his trunk and face, bruises after the gentlest knock, and has developed purple stretch marks across his abdomen and new diabetes. Down the corridor a young man is recovering from an episode that frightened him badly: a sudden pounding headache, drenching sweat, a thumping heart and a blood pressure that briefly touched 220/120 before settling. Three patients, three very different presentations — and yet all three may be explained by a gland the size of a thumbnail sitting on top of a kidney. The clinical art is to hear each story, name the hormone behind it, and trace it back to its source before a knife ever comes near the retroperitoneum.
WHY THIS MATTERS
Adrenal disorders matter to the surgeon for two reasons. First, several of them are eminently curable: a single autonomously functioning adenoma removed by laparoscopic adrenalectomy can cure resistant hypertension or reverse a metabolic catastrophe. Second, they are dangerous precisely when they are not recognised — an undiagnosed phaeochromocytoma taken to theatre for an unrelated operation can throw a fatal hypertensive crisis on induction or on handling of the tumour. The adrenal also illustrates a principle that runs through all of endocrine surgery: you confirm the biochemical diagnosis first, localise second, and operate last, never the other way round. For a final-year student, adrenal disease is also where the basic-science zones of the cortex and the catecholamine-secreting medulla finally pay off as bedside reasoning — each clinical syndrome maps onto a specific layer of the gland.
RECALL
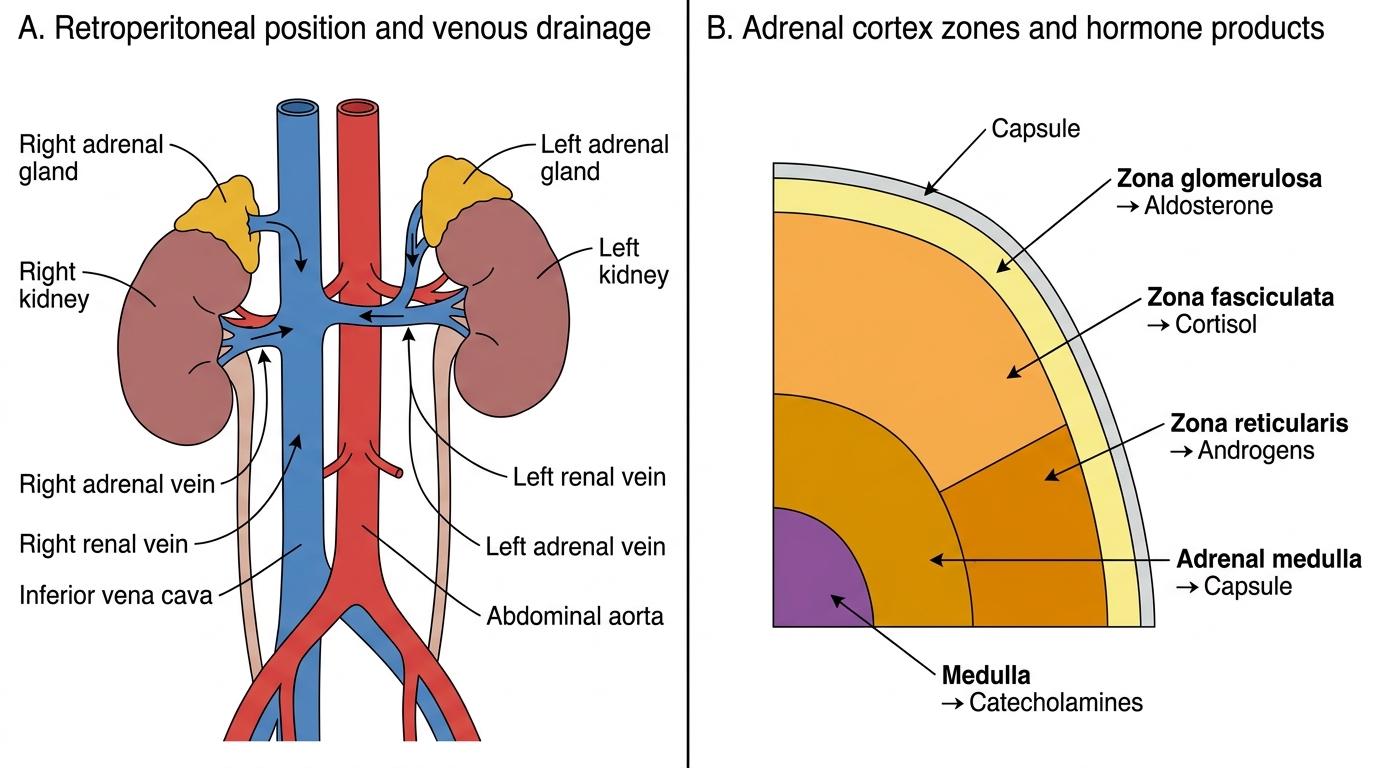
Recall the structure of the gland before we build clinical reasoning on it. Each adrenal is a retroperitoneal organ capping the upper pole of its kidney and is functionally two glands in one. The outer adrenal cortex is arranged in three zones, remembered by their products: the zona glomerulosa makes the mineralocorticoid aldosterone, the zona fasciculata makes the glucocorticoid cortisol, and the zona reticularis makes adrenal androgens — a useful mnemonic is that going from outside in the products are 'salt, sugar, sex'. The inner adrenal medulla is modified sympathetic tissue: its chromaffin cells secrete the catecholamines adrenaline and noradrenaline. Recall too that cortisol release is driven by pituitary ACTH within the hypothalamic-pituitary-adrenal axis, while aldosterone is controlled chiefly by the renin-angiotensin system and serum potassium. Hold these pairings in mind — every functional adrenal disorder is simply too much of one of these hormones.
The Patient with an Adrenal Disorder
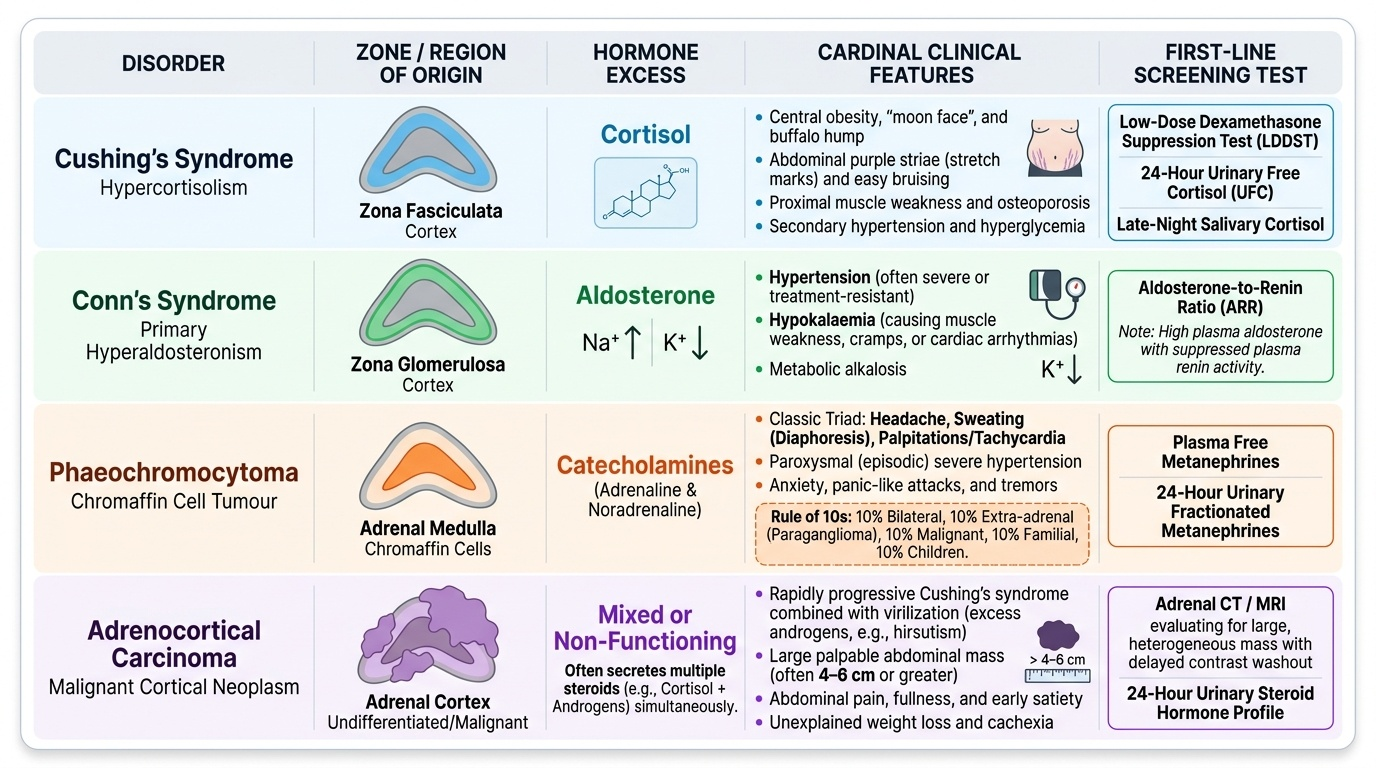
Adrenal disease reaches the surgeon by a small number of recognisable routes, and learning these clinical patterns is what lets you pick the right test. The commonest reason today is incidental: an adrenal incidentaloma, a mass found unexpectedly on a CT or MRI requested for something else entirely, which then has to be assessed for whether it is functioning and whether it is malignant. The classic functional presentations are the next route. Cortisol excess (Cushing's syndrome) produces central (truncal) obesity with a moon face and buffalo hump, thin easily-bruised skin with purple abdominal striae, proximal muscle weakness, new or worsened hypertension and diabetes, and in women hirsutism and menstrual disturbance. Aldosterone excess (Conn's syndrome) presents far more quietly, usually as resistant or early-onset hypertension, sometimes with the symptoms of hypokalaemia — muscle weakness, cramps and polyuria. Catecholamine excess (phaeochromocytoma) is the dramatic one: the classic triad of episodic headache, sweating and palpitations on a background of hypertension that may be sustained or paroxysmal, often with anxiety, pallor and tremor during an attack. A separate and worrying route is the patient with a large or rapidly growing adrenal mass with local symptoms — flank or back pain, or features of hormone excess of sudden onset — which raises the question of adrenocortical carcinoma. The history therefore does the early triage: it tells you which hormone to chase and how urgent the situation is.
Applied Anatomy and the Pathological Basis of Adrenal Disorders
Safe adrenal surgery is, once again, anatomy made practical. Each gland sits in the retroperitoneum on the upper pole of the kidney, enclosed in the perinephric (Gerota's) fascia. The arterial supply is rich and threefold — superior suprarenal arteries from the inferior phrenic artery, a middle suprarenal artery directly from the aorta, and inferior suprarenal arteries from the renal artery — so haemostasis during dissection demands care. The venous drainage is the surgically critical asymmetry: the right adrenal vein is short and drains directly into the inferior vena cava, which makes right adrenalectomy technically more demanding and bleeding more dangerous, whereas the left adrenal vein is longer and drains into the left renal vein. Pathologically, the disorders simply follow the histology. From the cortex, excess cortisol from the zona fasciculata (an adrenal adenoma, or driven by pituitary or ectopic ACTH) causes Cushing's syndrome; excess aldosterone from the zona glomerulosa (most often an aldosterone-producing adenoma) causes Conn's syndrome / primary hyperaldosteronism, the cardinal features of which are hypertension and hypokalaemia; and a malignant cortical tumour, adrenocortical carcinoma, may secrete a mixture of these hormones or be non-functioning but is characterised by a large, often >4–6 cm, irregular mass. From the medulla, a catecholamine-secreting tumour of chromaffin cells is a phaeochromocytoma, classically described by the 'rule of 10s' — roughly 10% bilateral, 10% extra-adrenal (then called a paraganglioma), 10% malignant, 10% familial (e.g. with MEN-2, von Hippel–Lindau or neurofibromatosis), and 10% occurring in children.
Provided image
Adrenal Gland Anatomy, Zones, Hormones, and Venous Drainage
| Disorder | Hormone excess | Origin | Cardinal features | Screening test |
|---|---|---|---|---|
| Cushing's syndrome | Cortisol | Zona fasciculata (cortex) | Truncal obesity, moon face, striae, bruising, diabetes, hypertension | Overnight 1 mg dexamethasone suppression test |
| Conn's syndrome | Aldosterone | Zona glomerulosa (cortex) | Resistant hypertension + hypokalaemia | Aldosterone:renin ratio |
| Phaeochromocytoma | Catecholamines | Medulla (chromaffin cells) | Episodic headache, sweating, palpitations + hypertension | Plasma/urinary metanephrines |
| Adrenocortical carcinoma | Mixed/none | Cortex (malignant) | Large mass, rapid growth, mixed hormone excess | Imaging + hormone panel |
SELF-CHECK
Which surgical anatomical fact makes RIGHT adrenalectomy more hazardous than left?
A. The right adrenal vein is short and drains directly into the inferior vena cava
B. The right adrenal has no arterial supply
C. The right adrenal vein drains into the left renal vein
D. The right adrenal lies anterior to the pancreas
Reveal Answer
Answer: A. The right adrenal vein is short and drains directly into the inferior vena cava
The right adrenal vein is short and enters the inferior vena cava directly, so avulsion or a torn stump risks major caval haemorrhage; this makes right adrenalectomy technically more demanding. The LEFT adrenal vein is longer and drains into the left renal vein.
Examination and Investigation of Adrenal Disease
Examination is targeted by the suspected syndrome but always includes the basics: a reliable blood pressure (lying and standing, looking for the paroxysms or resistant elevation of phaeochromocytoma and Conn's), the Cushingoid habitus (moon face, buffalo hump, truncal obesity, proximal myopathy on standing from a chair, thin skin, purple striae and bruising), and a search for clues to a syndromic or familial cause. The cardinal rule of investigation is to confirm the hormonal syndrome biochemically FIRST, and only then localise — because finding an adrenal mass on a scan tells you nothing about whether it is the source of the problem, and chasing an image before the biochemistry leads to wrong operations. For suspected cortisol excess, screen with the overnight 1 mg dexamethasone suppression test (failure of morning cortisol to suppress is positive), supported by late-night salivary cortisol or 24-hour urinary free cortisol, then use ACTH and further testing to separate ACTH-dependent from ACTH-independent causes. For suspected aldosterone excess, screen with the aldosterone:renin ratio (a high ratio with hypokalaemia suggests primary hyperaldosteronism), confirm with a suppression test, and use adrenal vein sampling to lateralise before surgery. For suspected phaeochromocytoma, the most sensitive screen is plasma free metanephrines or 24-hour urinary fractionated metanephrines. Only once the syndrome is confirmed do you localise with cross-sectional imaging — a dedicated adrenal-protocol CT or MRI — adding functional imaging (e.g. MIBG scintigraphy for phaeochromocytoma) where needed. For an incidentaloma, the same logic applies in reverse: every incidentaloma is screened for function (a dexamethasone suppression test, metanephrines, and ARR if hypertensive) and assessed for malignant risk by size and imaging characteristics.
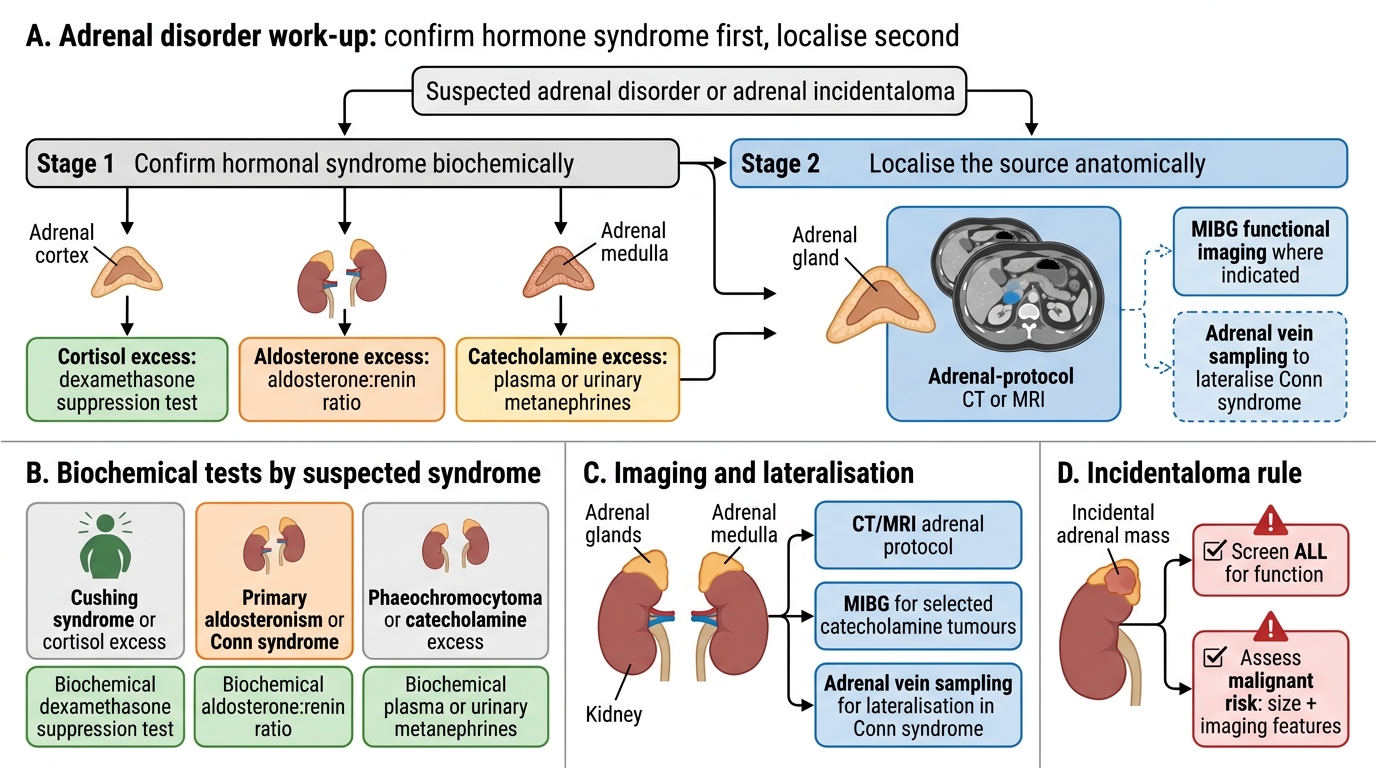
Adrenal Disorder Work-up: Confirm First, Localise Second
- Confirm the syndrome first: dexamethasone suppression (cortisol); aldosterone:renin ratio (aldosterone); metanephrines (catecholamines).
- Localise second: adrenal-protocol CT/MRI; functional imaging (MIBG) where indicated; adrenal vein sampling to lateralise Conn's.
- Incidentaloma: screen ALL for function + assess malignant risk by size and imaging features.