Page 4 of 17
SU23.3 | Adrenal Tumors — SDL Guide
Learning Objectives
- Classify adrenal tumours into cortical (benign adenoma vs adrenocortical carcinoma), medullary (phaeochromocytoma and paraganglioma) and secondary (metastatic) lesions, and distinguish functioning from non-functioning tumours (SU23.3).
- Describe the principles of investigation of an adrenal tumour, framed as the two parallel questions: is it functioning, and is it malignant (SU23.3).
- Outline the principles of management of adrenal tumours — surveillance, laparoscopic or radical adrenalectomy, and oncological follow-up — based on size, function and malignant risk (SU23.3).
INSTRUCTIONS
Modern cross-sectional imaging finds adrenal masses constantly, most of them silent and harmless, a few of them dangerous. The surgeon's job with any adrenal tumour is to answer two questions at once and never to confuse them: is this lump making a hormone, and is this lump a cancer? A tumour can be functioning and benign, non-functioning and benign, functioning and malignant, or non-functioning and malignant — and the management follows from where the answer lands on that grid. This module builds on the adrenal anatomy and functional syndromes you have already met and turns them into a clean decision framework for the adrenal mass, including the rules that keep a patient safe: screen for catecholamines before you ever biopsy, and never biopsy what is probably a primary adrenal cancer.
References
- Bailey & Love's Short Practice of Surgery, The Adrenal Glands and Other Abdominal Endocrine Disorders (textbook)
- SRB's Manual of Surgery, Adrenal Gland and Adrenal Tumours (textbook)
- Sabiston Textbook of Surgery, The Adrenal Gland (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old man has a CT scan of his abdomen after a road traffic accident. He has no symptoms referable to his adrenals, but the radiologist notes, almost in passing, a 3-centimetre mass on his left adrenal gland. He feels perfectly well and wants to know why anyone is worried about something found by accident. In a different clinic, a 40-year-old woman has an 8-centimetre right adrenal mass that has grown noticeably over a few months, along with new hypertension, weight gain and signs of androgen excess. The same organ, two completely different problems: one almost certainly a harmless incidentaloma that needs only the right screening and a plan, the other a mass whose size, growth and mixed hormone output shout adrenocortical carcinoma. Knowing how to tell these apart — and what to do next for each — is the whole of adrenal tumour surgery.
WHY THIS MATTERS
Adrenal tumours matter because the stakes range from 'reassure and discharge' to 'this is a rare and aggressive cancer'. Get the framework right and you spare the well patient an unnecessary operation while catching the rare malignancy early enough to act. Get it wrong and you either operate on harmless adenomas or, far worse, miss an adrenocortical carcinoma or send an unprepared phaeochromocytoma patient into theatre. There are also two safety rules unique to this organ that every clinician must internalise: you screen any adrenal mass for catecholamine excess before any intervention because biopsying or operating on an unsuspected phaeochromocytoma can trigger a fatal crisis, and you generally do NOT biopsy a suspected primary adrenal tumour because it rarely changes management and can seed a cancer. For a final-year student, the adrenal tumour is the cleanest example in surgery of a two-axis decision — functioning or not, malignant or not — and learning to hold both questions at once is the skill being tested.
RECALL
Recall the foundations from the preceding work on the adrenal gland. The adrenal cortex has three zones whose products are aldosterone, cortisol and androgens, while the adrenal medulla secretes catecholamines from chromaffin cells. The functional syndromes you already know — Cushing's (cortisol), Conn's (aldosterone) and phaeochromocytoma (catecholamines) — are each caused by a tumour or hyperplasia of the corresponding tissue, so a 'functioning' adrenal tumour simply means one that is producing one of these hormones in excess. Recall too the surgical anatomy that governs any adrenalectomy: the retroperitoneal position, the rich arterial supply, and the asymmetric venous drainage in which the short right adrenal vein drains directly into the inferior vena cava. Finally, hold on to the phaeochromocytoma 'rule of 10s' and the alpha-blockade-before-beta-blockade rule, because they reappear the moment a catecholamine-secreting tumour is the lump in question.
The Patient with an Adrenal Tumour
Adrenal tumours come to attention by three broad routes, and recognising which route a patient has taken sets the urgency and the work-up. The commonest by far is the adrenal incidentaloma — a mass discovered on a CT or MRI performed for an unrelated reason, in a patient with no adrenal symptoms at all, exactly like the man scanned after his accident. Such patients feel well and are often puzzled by the concern, but every incidentaloma still has to be assessed, because a minority are functioning or malignant. The second route is the functioning tumour that declares itself through its hormone: a patient who presents with Cushing's syndrome, Conn's syndrome or the paroxysmal headache–sweating–palpitations of a phaeochromocytoma, in whom imaging then reveals the responsible adrenal tumour. The third and most worrying route is the large or rapidly growing mass with features that suggest malignancy — a tumour several centimetres across that has grown over weeks to months, sometimes with flank or back pain from local invasion, sometimes with the rapid onset of mixed hormone excess (cortisol plus androgens, producing virilisation in a woman), which is the classic story of an adrenocortical carcinoma. A fourth possibility, especially in a patient with a known primary elsewhere, is an adrenal metastasis from a lung, breast, renal or melanoma primary. The history and the context therefore triage the patient long before the detailed biochemistry returns.
Classification and Pathological Basis of Adrenal Tumours
Adrenal tumours are best classified by their region of origin and their behaviour, and this classification drives everything that follows. Cortical tumours arise from the adrenal cortex. The benign adrenocortical adenoma is by far the commonest adrenal tumour; it may be functioning (secreting cortisol to cause Cushing's syndrome, or aldosterone to cause Conn's syndrome) or non-functioning (the typical small lipid-rich incidentaloma). Its malignant counterpart, the adrenocortical carcinoma (ACC), is rare but aggressive, tends to be large (often greater than 6 cm) at diagnosis, frequently secretes a mixture of hormones (cortisol with androgens being characteristic), and may invade locally or metastasise. Medullary tumours arise from chromaffin tissue: the phaeochromocytoma secretes catecholamines and follows the 'rule of 10s' (roughly 10% bilateral, 10% extra-adrenal, 10% malignant, 10% familial and 10% in children), and its extra-adrenal counterpart along the sympathetic chain is termed a paraganglioma. Finally, the adrenal is a common site of secondary metastases from primaries in the lung, breast, kidney and skin (melanoma). The crucial conceptual point is that two independent axes describe any adrenal tumour: whether it is functioning (hormone-secreting) and whether it is malignant (a cancer). These axes are independent — a tumour can be functioning yet benign, or non-functioning yet malignant — and the benign-versus-malignant judgement rests chiefly on size, growth rate, imaging characteristics and hormone profile rather than on biopsy.
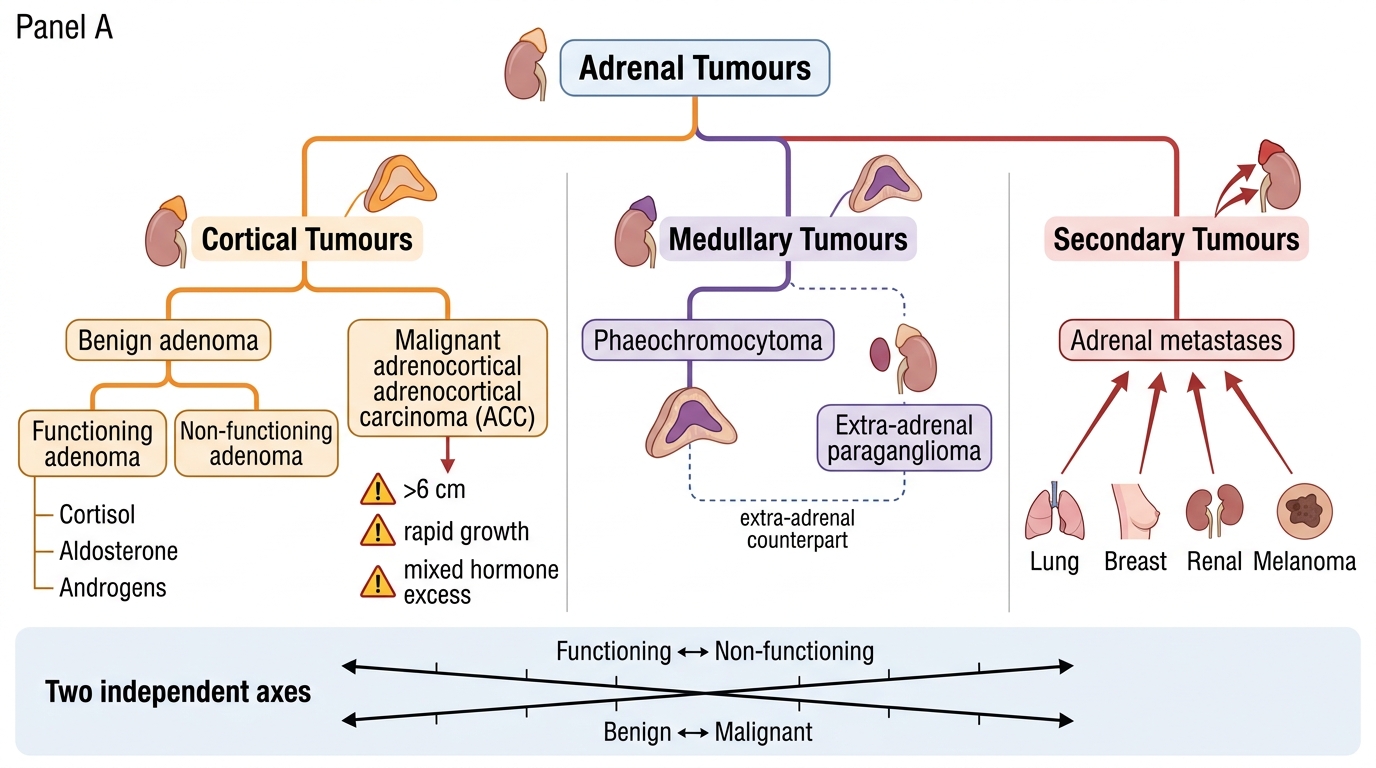
Classification of Adrenal Tumours
- Cortical: benign adenoma (functioning or non-functioning) vs malignant adrenocortical carcinoma (ACC).
- Medullary: phaeochromocytoma (extra-adrenal counterpart = paraganglioma).
- Secondary: metastases (lung, breast, renal, melanoma).
- Two independent axes: functioning vs non-functioning; benign vs malignant.
SELF-CHECK
A 9 cm adrenal mass has grown over three months and secretes both cortisol and androgens, causing Cushingoid features and virilisation in a woman. Which tumour does this picture most strongly suggest?
A. A small non-functioning adenoma
B. An adrenocortical carcinoma
C. A simple adrenal cyst
D. A benign aldosterone-producing adenoma
Reveal Answer
Answer: B. An adrenocortical carcinoma
Large size (>6 cm), rapid growth, and MIXED hormone excess (cortisol plus androgens producing virilisation) are the classic features of adrenocortical carcinoma. A benign adenoma is usually small and, if functioning, typically secretes a single hormone; a non-functioning adenoma causes no syndrome.
Principles of Investigation
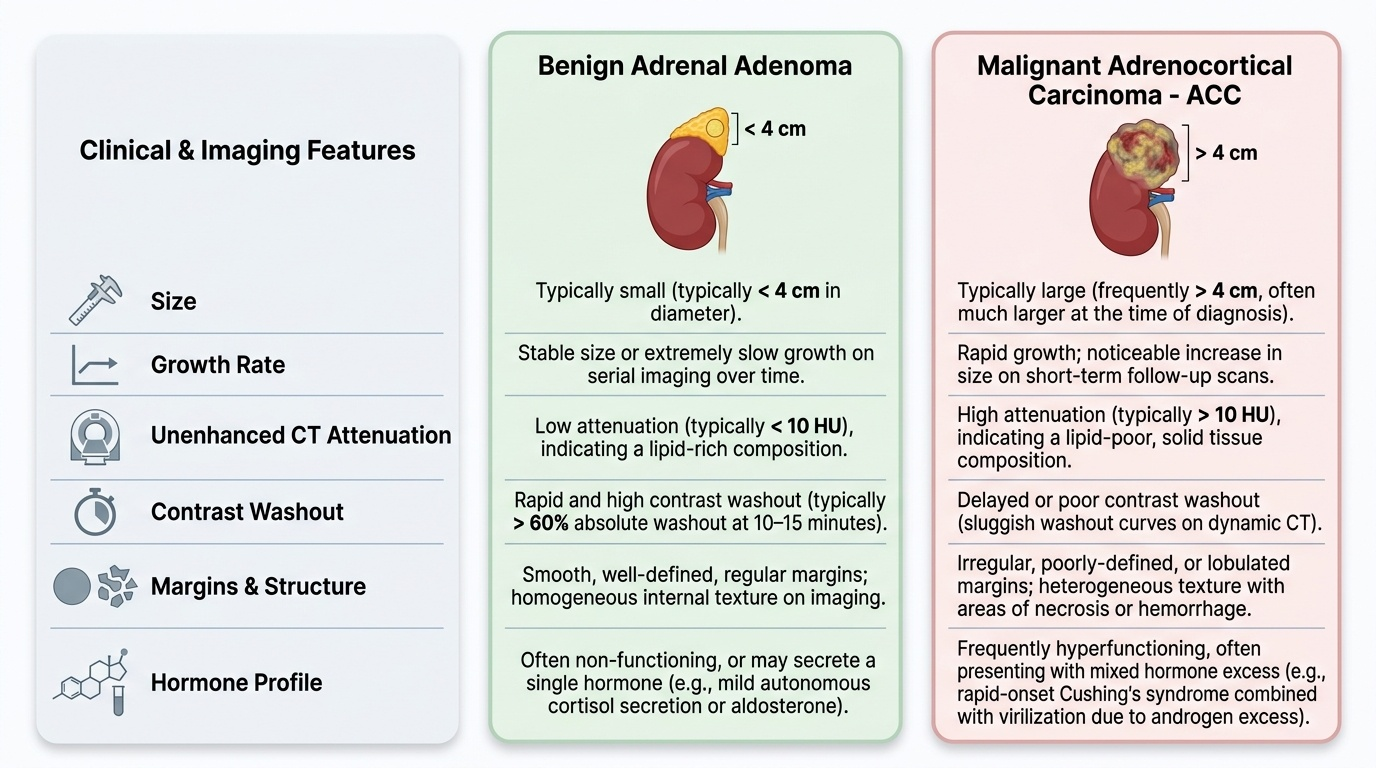
The investigation of any adrenal tumour is structured around the two parallel questions, and it is essential never to let one answer stand in for the other. The first question — is it functioning? — is answered biochemically, and every adrenal mass is screened regardless of symptoms: an overnight 1 mg dexamethasone suppression test for autonomous cortisol secretion, plasma free or 24-hour urinary fractionated metanephrines for catecholamine excess, and, in any patient who is hypertensive, an aldosterone:renin ratio for primary hyperaldosteronism. The second question — is it malignant? — is answered chiefly by size and imaging characteristics: a small lesion is much more likely benign, while a mass greater than about 4 cm raises concern and an ACC is typically large at diagnosis, and growth on serial imaging is itself a worrying sign. On unenhanced CT, a lipid-rich benign adenoma characteristically has low attenuation (typically below about 10 Hounsfield units), whereas high attenuation, irregular margins, heterogeneity and poor contrast washout point towards malignancy or a phaeochromocytoma. A critical safety rule governs tissue sampling: biopsy of an adrenal mass is generally avoided, both because it is rarely needed for a suspected primary adrenal tumour (and can seed an adrenocortical carcinoma) and because a phaeochromocytoma must be excluded by metanephrines before any needle or operation, since sampling an unsuspected phaeochromocytoma can precipitate a catecholamine crisis. Biopsy is reserved for the specific situation of confirming a suspected metastasis in a patient with a known extra-adrenal primary, and only after phaeochromocytoma has been excluded.
Provided image
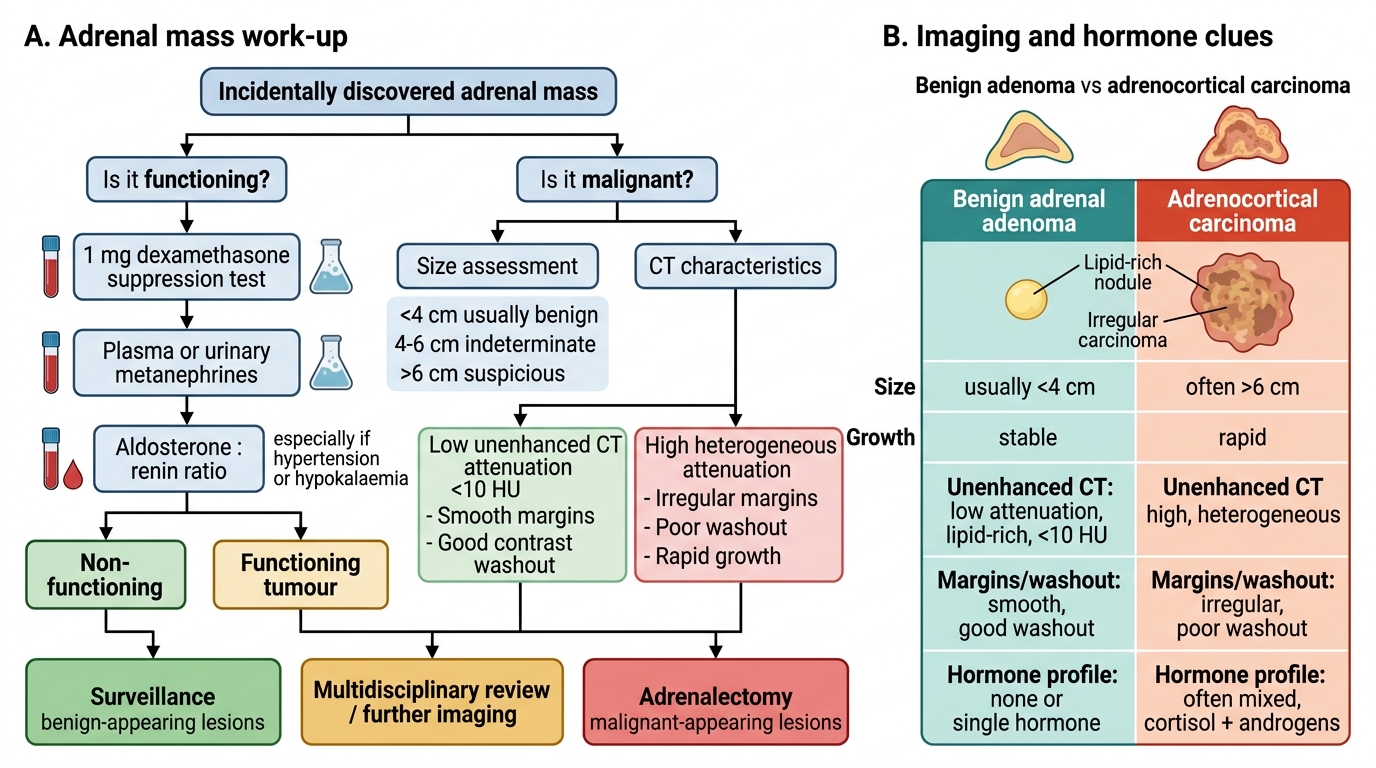
Adrenal Mass Work-Up
| Feature | Benign adenoma | Adrenocortical carcinoma |
|---|---|---|
| Size | Usually small (<4 cm) | Often large (>6 cm) |
| Growth | Stable | Rapid |
| Unenhanced CT attenuation | Low (lipid-rich, ~<10 HU) | High, heterogeneous |
| Margins/washout | Smooth, good washout | Irregular, poor washout |
| Hormone profile | None or single hormone | Often mixed (cortisol + androgens) |