Page 2 of 17
SU25.1 | Breast Anatomy and Investigation — SDL Guide (Part 2)
Choosing and Interpreting Breast Investigations
Selecting the right imaging is mostly a question of breast density, which falls with age. In younger women (typically under 35 years) the breast is glandular and dense, so a mammogram is hard to read and ultrasound is the first-line imaging; it is excellent at distinguishing a solid mass from a simple cyst and is the modality of choice in pregnancy. In older women (typically over 35-40 years) the breast is more fatty and mammography becomes the first-line test, detecting masses, architectural distortion and the microcalcifications that can be the only sign of an early or in-situ cancer; ultrasound is then used as a targeted adjunct. (Note that population mammographic screening of asymptomatic women is a separate activity, typically offered around 50-69 years; the age rules here concern symptomatic work-up.) Imaging is reported with the standardised BI-RADS system (categories 0-6): 0 = incomplete/needs further imaging; 1 = negative; 2 = benign; 3 = probably benign (low malignancy risk, short-interval follow-up); 4 = suspicious (biopsy indicated); 5 = highly suggestive of malignancy; 6 = biopsy-proven malignancy. The pathology arm should wherever possible be a core needle biopsy, because it yields a tissue histology sample that distinguishes invasive from in-situ disease and provides receptor status (ER/PR/HER2) needed for treatment; FNAC gives only cytology and cannot make that distinction, so core biopsy is generally preferred. MRI is reserved for specific situations such as assessing lobular cancers, implants, the high-risk (e.g. BRCA-carrier) breast and equivocal cases.
Provided image
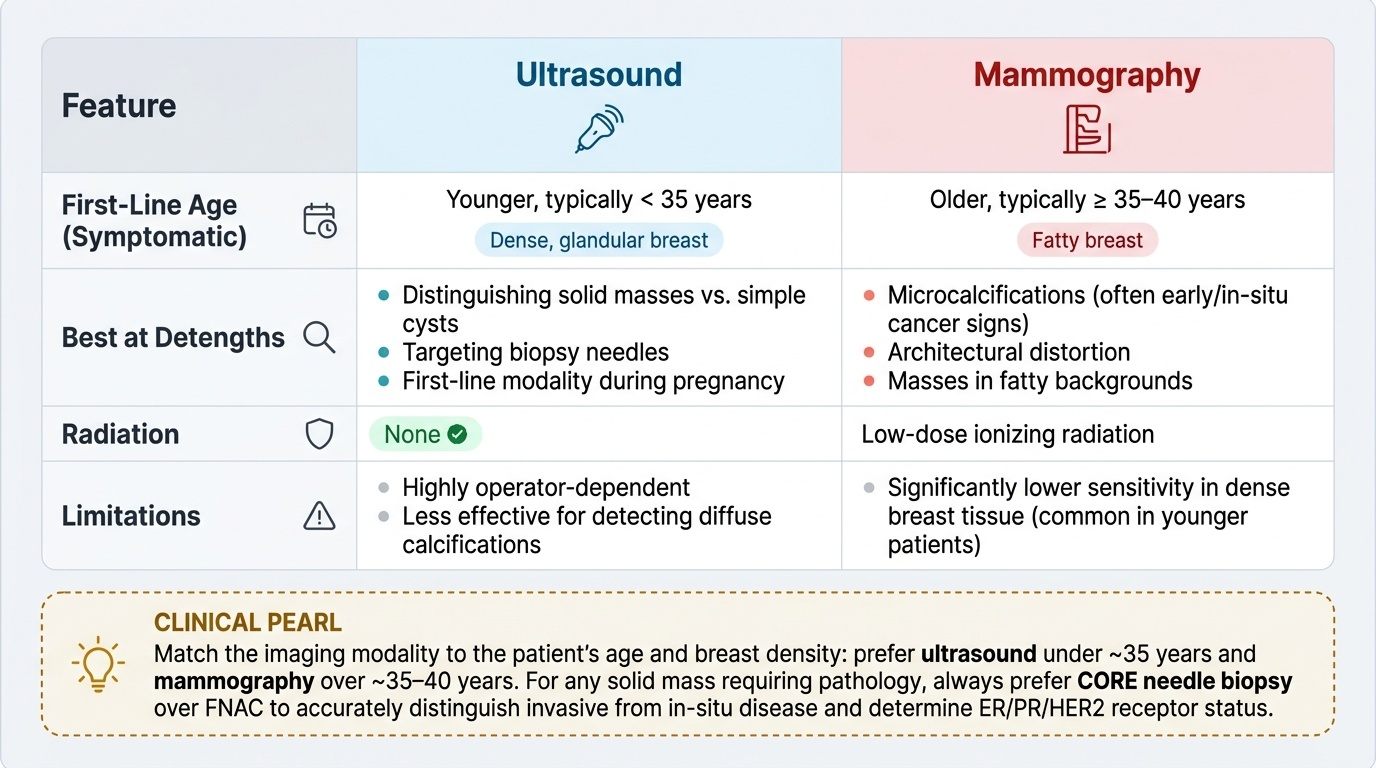
| Feature | Ultrasound | Mammography |
|---|---|---|
| First-line age (symptomatic) | Younger, typically <35 y (dense breast) | Older, typically >35-40 y (fatty breast) |
| Best at | Solid vs cystic, targeting biopsy, pregnancy | Microcalcifications, architectural distortion |
| Radiation | None | Low-dose ionising |
| Limitation | Operator-dependent; less good for diffuse calcification | Less sensitive in dense/young breast |
CLINICAL PEARL
Match the imaging to the age and density, and prefer CORE biopsy over FNAC for a solid mass. In a woman under ~35, ultrasound is first-line because mammography is hard to read in a dense breast; over ~35-40, mammography leads because it shows microcalcifications that ultrasound misses. And reach for a CORE needle biopsy rather than FNAC whenever you can: only histology distinguishes invasive from in-situ cancer and provides ER/PR/HER2 receptor status, which directly shapes treatment. FNAC gives cytology alone and cannot make these distinctions.
Check Your Understanding
Bring the threads together by reasoning through the two women in the hook. The 24-year-old with a smooth, mobile, slipping lump is statistically and clinically likely to have a benign fibroadenoma: triple assessment for her means clinical examination, ultrasound (because her breast is dense) and, if the lump is solid, a core biopsy — concordant benign results would justify reassurance. The 58-year-old with a hard, irregular, skin-puckering lump sits at the malignant end: skin dimpling implies Cooper's-ligament tethering, and her work-up is clinical examination, mammography with targeted ultrasound, and a core biopsy for histology and receptor status. Use these to self-test the competency. First, can you name the anatomical facts that explain skin dimpling (Cooper's ligaments), deep fixity (retromammary space) and where most cancers arise (upper outer quadrant/axillary tail)? Second, can you describe the lymphatic drainage and the level I/II/III axillary framework? Third, can you state the components of triple assessment, choose ultrasound versus mammography by age, read a BI-RADS category, and justify core biopsy over FNAC? The questions that follow check exactly these links.
SELF-CHECK
A 30-year-old woman presents with a discrete breast lump. Which is the most appropriate FIRST-LINE imaging investigation?
A. Mammography
B. Ultrasound
C. MRI of the breast
D. CT chest
Reveal Answer
Answer: B. Ultrasound
In a woman under about 35 years the breast is glandular and dense, which makes mammograms difficult to interpret; ULTRASOUND is therefore first-line and reliably distinguishes a solid mass from a simple cyst. Mammography becomes first-line in older (>35-40 y) women with fattier breasts. MRI is reserved for specific indications, and CT has no role in primary breast lump assessment.