Page 8 of 17
SU25.3-4 | Breast Tumours and Malignancy Counselling — SDL Guide (Part 2)
Principles of Treatment: Surgery, Axilla and Adjuvant Therapy
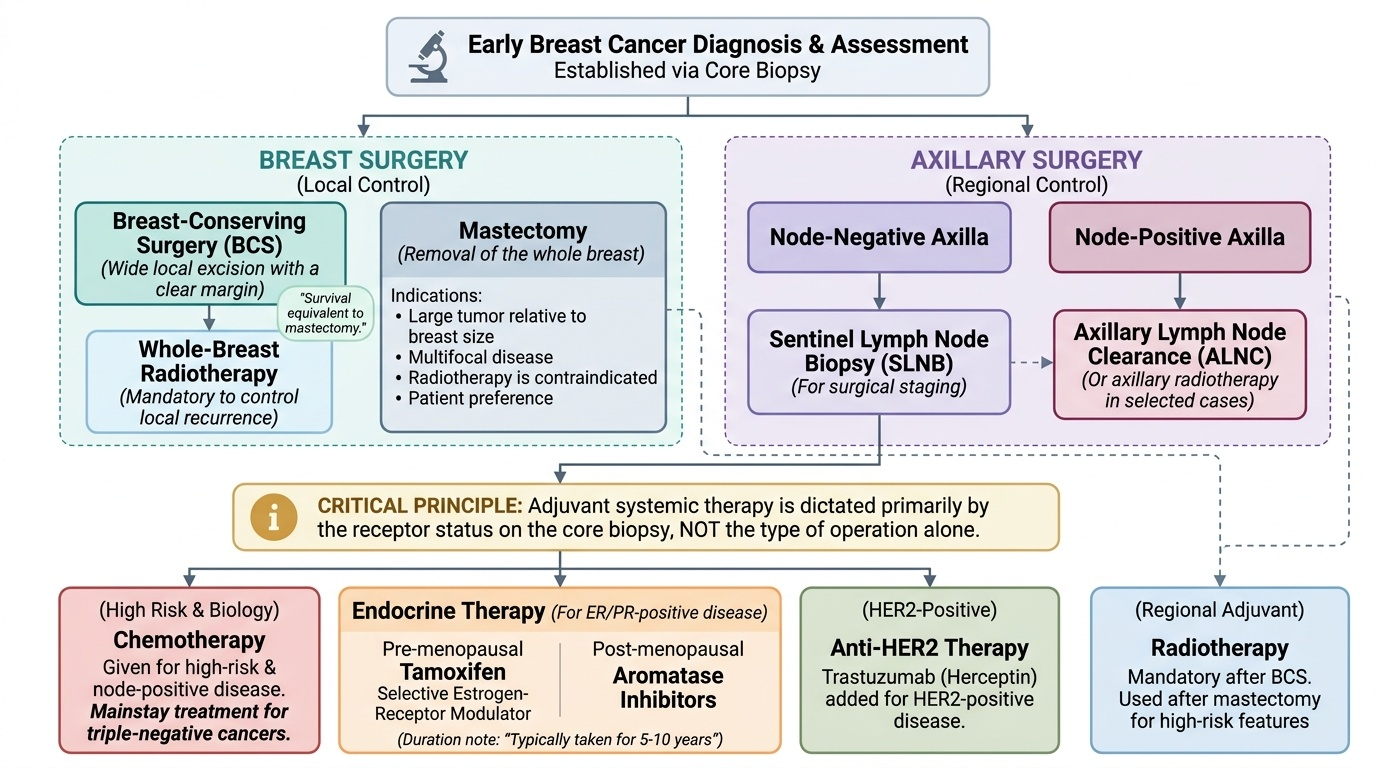
Modern breast cancer treatment is multimodal and individualised by stage and biology, planned in a multidisciplinary team. Local surgery to the breast offers two main options. Breast-conserving surgery (BCS) — a wide local excision of the tumour with a clear margin — is suitable for many early cancers and gives a survival equivalent to mastectomy, but it must always be combined with whole-breast radiotherapy to control local recurrence. Mastectomy (removal of the whole breast, with reconstruction options) is chosen for large tumours relative to breast size, multifocal disease, when radiotherapy is contraindicated, or by patient preference. Axillary surgery runs in parallel: a node-negative axilla is staged by sentinel lymph node biopsy, while a node-positive axilla is treated by axillary clearance (or, in selected cases, axillary radiotherapy). Adjuvant (and sometimes neoadjuvant) therapy then targets micrometastatic and residual disease according to biology and stage. Radiotherapy is mandatory after BCS and used after mastectomy for high-risk features. Chemotherapy is given for higher-risk and node-positive disease and is the mainstay for triple-negative cancers. Endocrine therapy is given for ER/PR-positive disease — tamoxifen (a selective oestrogen-receptor modulator) is used particularly in pre-menopausal women, and aromatase inhibitors in post-menopausal women — typically for several years. Anti-HER2 therapy (trastuzumab) is added for HER2-positive disease. The point students must grasp is that the receptor status on the core biopsy, not the operation alone, dictates much of this systemic plan.
Provided image
- Breast surgery: BCS (wide local excision) + whole-breast radiotherapy = survival equivalent to mastectomy; or mastectomy for large/multifocal disease or preference.
- Axilla: SLNB (node-negative) vs axillary clearance (node-positive).
- Adjuvant by biology: chemotherapy (high-risk/node-positive; mainstay for triple-negative); endocrine therapy for ER/PR-positive (tamoxifen pre-menopausal, aromatase inhibitor post-menopausal); trastuzumab for HER2-positive.
SELF-CHECK
A woman with early breast cancer suitable for breast-conserving surgery asks whether keeping her breast means a worse chance of cure. What is the correct principle to convey?
A. Mastectomy always gives better survival than breast conservation
B. Breast-conserving surgery gives equivalent survival to mastectomy, provided it is combined with whole-breast radiotherapy
C. Breast-conserving surgery never needs radiotherapy
D. Survival depends only on the operation, not on the tumour biology
Reveal Answer
Answer: B. Breast-conserving surgery gives equivalent survival to mastectomy, provided it is combined with whole-breast radiotherapy
For suitable early breast cancers, breast-conserving surgery (wide local excision) gives SURVIVAL EQUIVALENT to mastectomy, but it must ALWAYS be combined with whole-breast radiotherapy to keep local recurrence low. Overall outcome also depends heavily on tumour biology and stage (receptor status, grade, nodes), not the operation alone.
Counselling and Informed Consent for Treatment of Breast Cancer
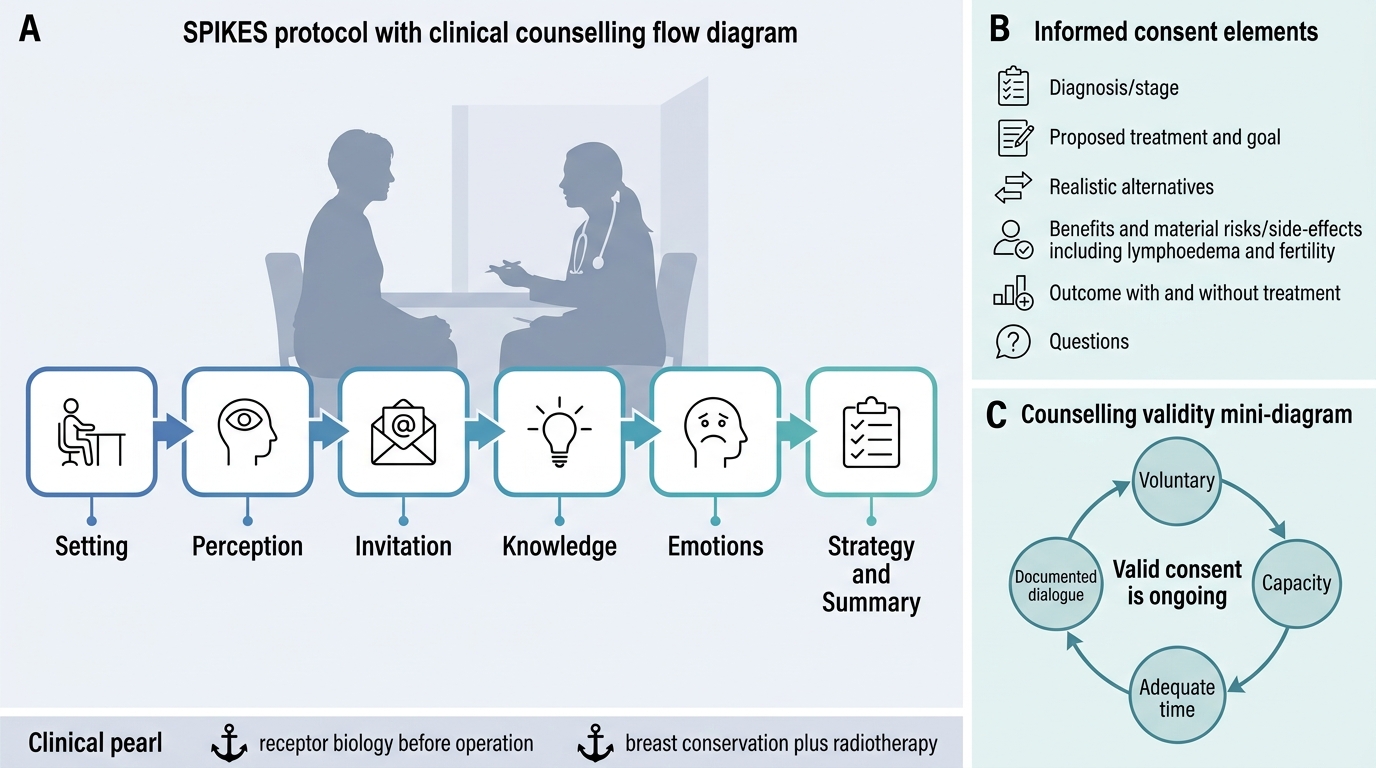
Counselling a woman with breast cancer and obtaining her informed consent is a structured clinical skill, not an afterthought, and competency SU25.4 requires you to be able to do it. Breaking the bad news is best done with a recognised framework such as SPIKES: prepare the Setting (a private, unhurried place, ideally with a relative or breast-care nurse present); assess the patient's Perception of what is happening; obtain her Invitation — how much she wants to know; give the Knowledge clearly, in plain language, with a warning shot, avoiding jargon and pausing often; respond to her Emotions with empathy and silence rather than rushing on; and agree a Strategy and Summary with a clear next step and written information. Informed consent for treatment then has specific elements you must cover and document: the diagnosis and stage in understandable terms; the proposed treatment and its goals (cure vs control); the realistic alternatives (for example BCS-plus-radiotherapy versus mastectomy, and the reconstruction options); the benefits and the material risks/side-effects of each (surgical complications, lymphoedema after axillary clearance, the side-effects of chemotherapy, radiotherapy and endocrine therapy, and effects on fertility in younger women); the likely outcome with and without treatment; and explicit space for questions. Consent must be voluntary and given by a patient with capacity, after enough time to decide, and it is a continuing dialogue rather than a single signature. Throughout, communicate honestly but with hope, respect the patient's autonomy, maintain confidentiality, and offer support resources — this human competence is as much a part of safe surgery as the operation itself.
SPIKES Protocol and Consent in Breast Oncology Counselling
- SPIKES: Setting → Perception → Invitation → Knowledge → Emotions → Strategy/Summary.
- Informed consent elements: diagnosis/stage; proposed treatment + goal; realistic alternatives; benefits + material risks/side-effects (incl. lymphoedema, fertility); outcome with/without; questions.
- Validity: voluntary, with capacity, adequate time; a continuing dialogue, documented.
CLINICAL PEARL
Two anchors keep breast oncology and counselling straight. First, biology before operation: the ER/PR/HER2 status on the core biopsy decides much of the systemic treatment — endocrine therapy for ER/PR-positive (tamoxifen in pre-menopausal, aromatase inhibitors in post-menopausal women), trastuzumab for HER2-positive, and chemotherapy as the mainstay for triple-negative disease — so a 'triple-negative' result is important news, not a footnote. Second, breast-conserving surgery is only equivalent to mastectomy WHEN it is paired with whole-breast radiotherapy; never quote conservation as 'just as good' without that radiotherapy caveat. And when you break the news, follow SPIKES and treat consent as an ongoing conversation, not a signature.
Check Your Understanding
Bring the threads together through the 52-year-old teacher from the hook. Her hard, irregular, skin-dimpling lump is suspicious for cancer; triple assessment with a core biopsy confirms an invasive carcinoma and — crucially — its grade and receptor status (ER/PR/HER2). She is staged by TNM, her clinically negative axilla assessed by sentinel lymph node biopsy, and her treatment planned multimodally: breast-conserving surgery with whole-breast radiotherapy (or mastectomy if unsuitable), with adjuvant therapy chosen by biology — endocrine therapy if ER/PR-positive, trastuzumab if HER2-positive, chemotherapy if high-risk or triple-negative. Then you must counsel her using SPIKES and obtain informed consent that covers her diagnosis, the proposed treatment and alternatives, the material risks and side-effects, and her questions. Use this to self-test the competencies. First, can you distinguish in-situ (DCIS/LCIS) from invasive cancer, name IDC/NST as commonest and ILC's multifocal tendency, and explain the treatment meaning of ER/PR, HER2 and triple-negative status? Second, can you outline TNM staging, the sentinel-node concept, and the principles of BCS-plus-radiotherapy versus mastectomy and the adjuvant therapies? Third, can you break bad news with SPIKES and list the elements of valid informed consent? The questions below check exactly these links.
SELF-CHECK
When breaking the news of a breast cancer diagnosis using the SPIKES framework, which action best reflects the 'E' step?
A. Booking the operating theatre before the patient arrives
B. Responding to the patient's distress with empathy and allowing silence
C. Quoting five-year survival statistics immediately after saying the word 'cancer'
D. Asking the patient to sign the consent form straight away
Reveal Answer
Answer: B. Responding to the patient's distress with empathy and allowing silence
In SPIKES, 'E' stands for Emotions: after delivering the knowledge, you respond to the patient's emotional reaction with empathy, acknowledgement and silence rather than rushing on with facts or logistics. Statistics and consent come later, once she is ready; pre-booking surgery or demanding an immediate signature ignores her autonomy and emotional state.