Page 7 of 14
SU26.4 | Lung Tumors — SDL Guide
Learning Objectives
- Describe the aetiology and pathogenesis of lung tumours, emphasising smoking, and outline their clinical features including paraneoplastic and special syndromes (SU26.4).
- Classify lung cancer into small-cell and non-small-cell types and explain why this distinction decides whether surgery has a role (SU26.4).
- Outline the principles of investigation, staging and management of lung cancer, including when surgical resection is appropriate (SU26.4).
INSTRUCTIONS
Lung cancer is one of the commonest and most lethal cancers, and almost all of it is caused by smoking — a fact that should colour everything from prevention to suspicion. For a surgeon-in-training the single most important idea is a dichotomy: lung cancer is either SMALL-CELL or NON-SMALL-CELL, and that one distinction, together with the stage, decides whether an operation can help at all. This module takes you from how a lung tumour presents — locally, by spread, and through curious paraneoplastic syndromes — through the classification and staging, to the principle that non-small-cell cancer is resected when it is early and the patient is fit, while small-cell cancer is treated medically. Keep the depth at 'knows': you are learning the principles of management, not how to perform a lobectomy.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 64-year-old lifelong smoker comes in with a cough that has changed in character over two months, streaks of blood in his sputum, and weight loss he cannot explain. His chest X-ray shows a mass near the centre of the right lung. In another room, a 58-year-old man complains of a deep, boring pain in his shoulder and arm; when you look at his face you notice that one eyelid droops and that pupil is small — and his chest X-ray shows a shadow right at the apex of the lung. Both men have lung tumours, but their stories, the cells involved, and crucially whether an operation can help them, may be entirely different. The reasoning that separates a tumour the surgeon can cure from one that belongs to the oncologist is what this module is about.
WHY THIS MATTERS
Lung cancer kills more people than almost any other malignancy, and because it is overwhelmingly caused by smoking it is both largely preventable and, sadly, often advanced by the time it is found. As a doctor you will meet it constantly: as a worrying chest X-ray, as a smoker with a persistent cough or haemoptysis, or as a strange constellation of symptoms from a paraneoplastic syndrome. Your job is to recognise the suspicion early, order the right work-up, and understand the one decision that governs everything — is this a tumour where surgery can offer cure, or one where chemotherapy and radiotherapy are the mainstay? Getting the small-cell versus non-small-cell distinction and the stage right is what protects patients from both futile operations and missed curative chances. Even at the knows level, this reasoning lets you counsel a frightened patient honestly about what their diagnosis means.
RECALL
Recall a few foundations before we build on them. From oncology in general: tumours are staged by the TNM system — the size and local extent of the primary Tumour, spread to regional lymph Nodes, and distant Metastases — and the stage, more than anything else, predicts prognosis and whether cure is possible. From anatomy and neurology: Horner's syndrome (ptosis, miosis and anhidrosis on one side of the face) results from interruption of the sympathetic supply to the eye and face. From physiology: some tumours secrete hormones or hormone-like substances, producing paraneoplastic syndromes — for example inappropriate antidiuretic hormone causing low sodium (SIADH), or ectopic adrenocorticotrophic hormone (ACTH) causing Cushing's features. Hold on to these three ideas — TNM staging, Horner's syndrome and paraneoplastic secretion — because each reappears as a key feature of lung cancer.
The Patient with a Suspected Lung Tumour
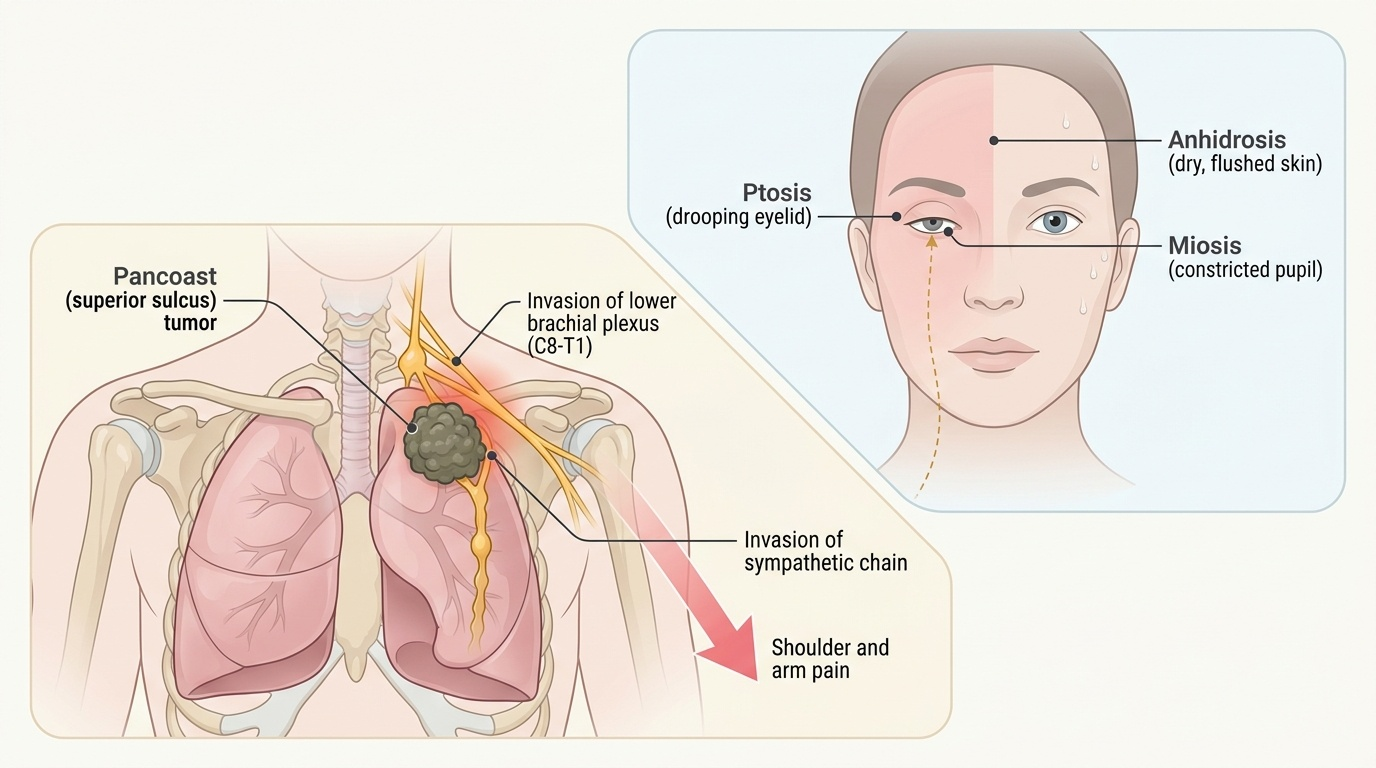
Lung tumours announce themselves in four overlapping ways, and a good history screens for all of them. The first is local (intrathoracic) disease from the tumour in the airway or chest: a new or changed cough, haemoptysis (coughing blood), breathlessness, chest pain, recurrent or non-resolving chest infection, and — if the tumour involves the recurrent laryngeal nerve — hoarseness, or, with mediastinal spread, superior vena cava obstruction. The second is metastatic disease, because lung cancer spreads early to liver, bone (pain, fractures), brain (headache, seizures, focal deficits) and adrenal glands, sometimes presenting through the metastasis rather than the lung. The third is paraneoplastic syndromes, distant effects of tumour-secreted substances: small-cell cancers classically cause SIADH (low sodium) and ectopic ACTH (Cushing's features), while squamous cell cancers classically cause hypercalcaemia through parathyroid-hormone-related peptide (PTHrP). The fourth is the special apical syndrome: a Pancoast (superior sulcus) tumour at the lung apex invades the sympathetic chain to cause Horner's syndrome (ptosis, miosis, anhidrosis) and the lower brachial plexus to cause shoulder and arm pain. General constitutional features — weight loss, anorexia, fatigue, finger clubbing — accompany many cases. Recognising which pattern a patient shows directs both suspicion and the work-up.
Provided image
- Local: cough, haemoptysis, breathlessness, chest pain, hoarseness, recurrent infection.
- Metastatic: liver, bone, brain, adrenal — may present through the metastasis.
- Paraneoplastic: small-cell → SIADH, ectopic ACTH; squamous → hypercalcaemia (PTHrP).
- Special: Pancoast tumour → Horner's syndrome + shoulder/arm pain.
Aetiology, Pathogenesis and the SCLC versus NSCLC Classification
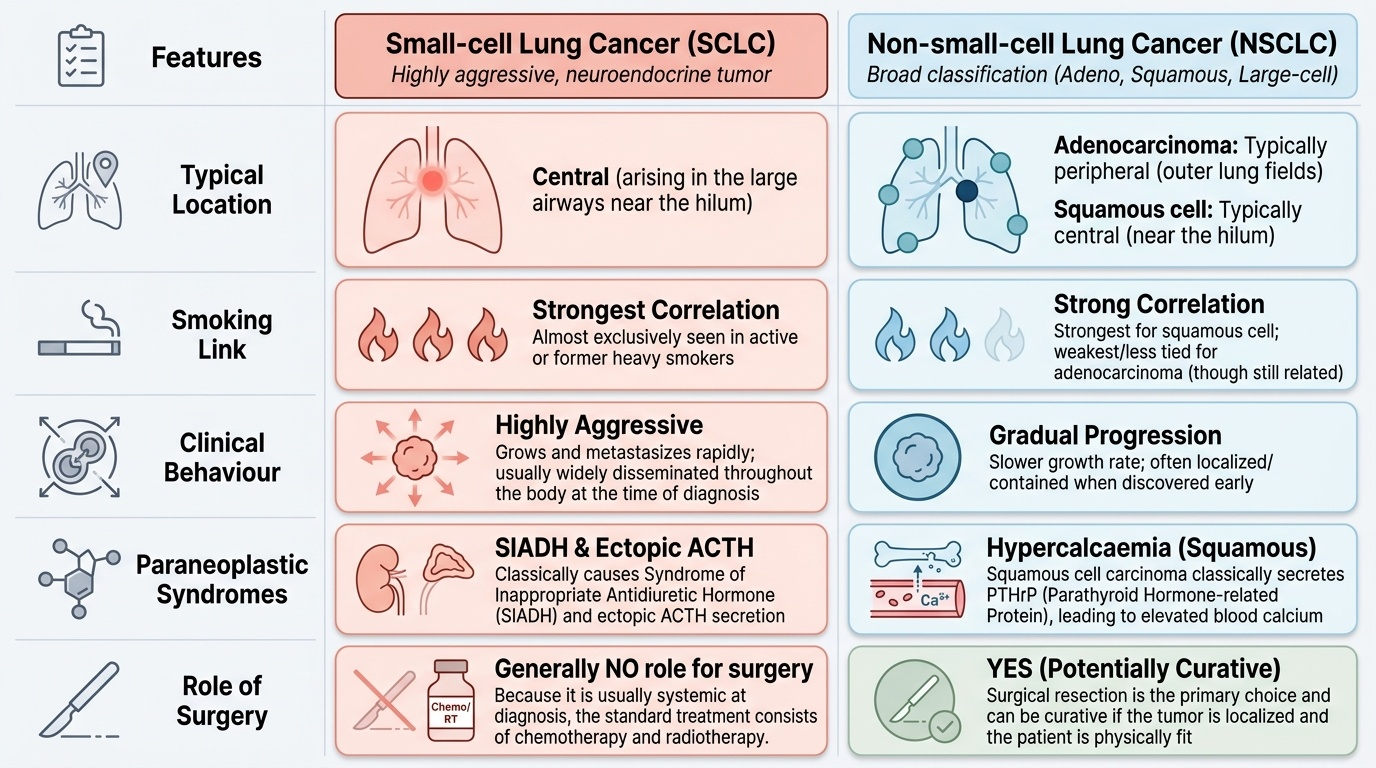
The dominant cause of lung cancer is cigarette smoking, which accounts for the great majority of cases through carcinogens that damage the bronchial epithelium and accumulate genetic mutations over years; the risk rises with the amount and duration of smoking and falls after cessation. Other contributors include passive smoking, radon, asbestos (which also causes mesothelioma), other occupational carcinogens, air pollution and prior lung disease. Most lung cancers arise from the bronchial epithelium and are therefore called bronchogenic carcinoma, and the surgically decisive step is to divide them into two groups. Small-cell lung cancer (SCLC) is a neuroendocrine tumour that is typically central (arising in the large airways near the hilum), is the most strongly smoking-related, grows and metastasises rapidly so that it is usually disseminated at diagnosis, and is the type that classically causes paraneoplastic SIADH and ectopic ACTH — for these reasons it is generally NOT a surgical disease and is treated with chemotherapy and radiotherapy. Non-small-cell lung cancer (NSCLC) is everything else and comprises three subtypes: adenocarcinoma (the commonest lung cancer overall, typically peripheral, and the type least tied to smoking though still smoking-related); squamous cell carcinoma (typically central, strongly smoking-related, may cavitate, and classically causes hypercalcaemia via PTHrP); and large-cell carcinoma. NSCLC is the group in which surgical resection can be curative when the tumour is localised and the patient is fit. This is why histology is requested before any operation is contemplated.
Provided image
| Feature | Small-cell (SCLC) | Non-small-cell (NSCLC) |
|---|---|---|
| Typical location | Central | Adenocarcinoma peripheral; squamous central |
| Smoking link | Strongest | Strong (weakest for adenocarcinoma) |
| Paraneoplastic | SIADH, ectopic ACTH | Squamous → hypercalcaemia (PTHrP) |
| Behaviour | Rapid, usually disseminated at diagnosis | Often localised when found early |
| Role of surgery | Generally NO (chemo/radiotherapy) | YES if localised and fit (resection can cure) |
SELF-CHECK
Why is the distinction between small-cell and non-small-cell lung cancer so important to a surgeon?
A. Small-cell cancer is usually resected surgically while non-small-cell is treated with chemotherapy
B. Small-cell cancer is generally treated with chemotherapy and radiotherapy (not surgery), whereas non-small-cell cancer can be cured by surgical resection if it is localised and the patient is fit
C. Both types are always treated identically, so the distinction is academic
D. The distinction only matters for predicting smoking history, not treatment
Reveal Answer
Answer: B. Small-cell cancer is generally treated with chemotherapy and radiotherapy (not surgery), whereas non-small-cell cancer can be cured by surgical resection if it is localised and the patient is fit
The small-cell versus non-small-cell split is the decisive surgical fork: small-cell lung cancer is usually disseminated at diagnosis and is treated with chemotherapy and radiotherapy, not surgery, whereas non-small-cell lung cancer can be cured by resection (lobectomy or pneumonectomy) when it is localised (early stage) and the patient is fit enough. Histology therefore determines whether an operation is even an option.
Investigation and Staging of Lung Cancer
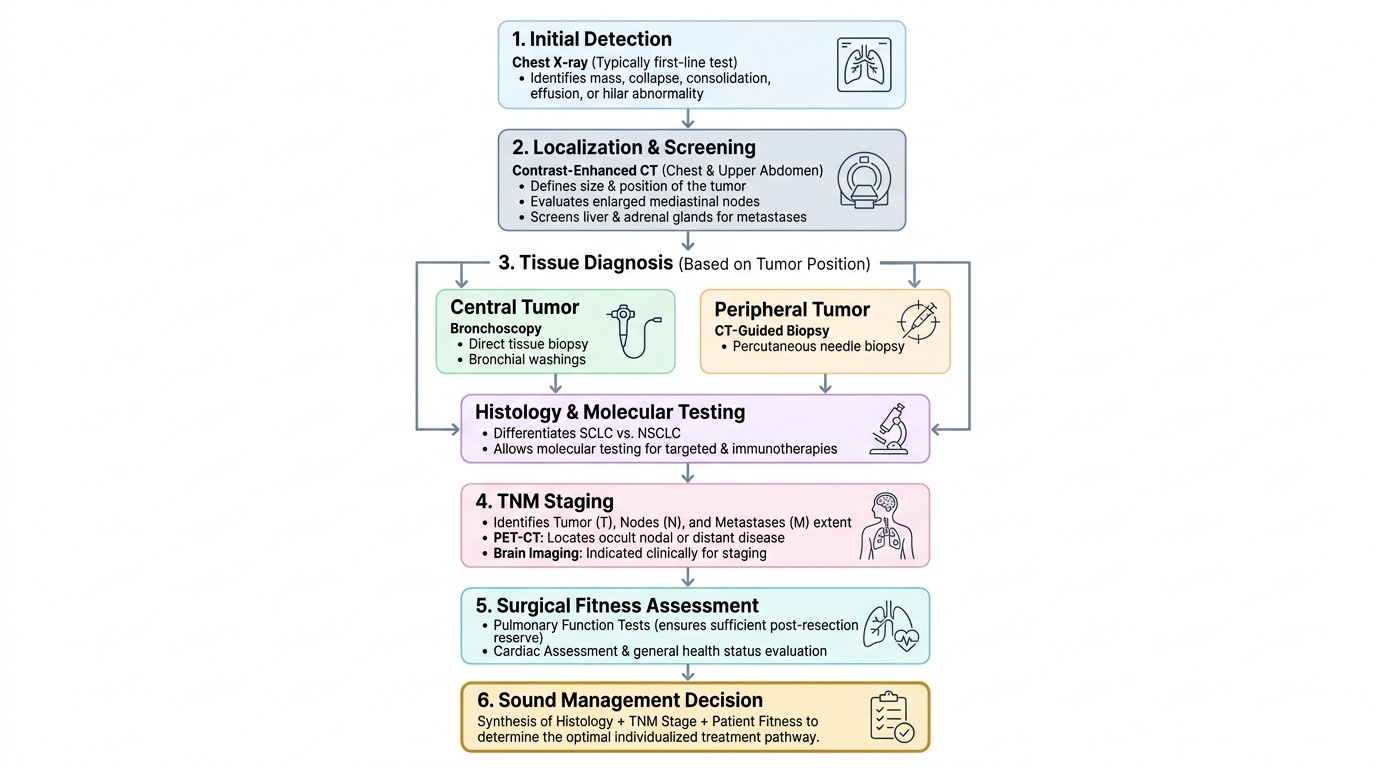
Investigation answers three questions in turn: is there a tumour, what type of cell is it, and how far has it spread — because only the answers together decide treatment. The chest X-ray is usually the first test and may show a mass, collapse, consolidation, an effusion or a hilar abnormality. The key cross-sectional test is contrast-enhanced computed tomography (CT) of the chest and upper abdomen, which defines the size and position of the tumour, looks for enlarged mediastinal nodes, and screens the liver and adrenals for metastases. A tissue diagnosis is essential and is obtained according to the tumour's position: a central tumour is reached by bronchoscopy with biopsy or washings, while a peripheral tumour is sampled by CT-guided percutaneous needle biopsy; this histology gives the all-important small-cell versus non-small-cell answer and, for NSCLC, allows molecular testing that may open targeted and immunotherapies. Staging then uses the TNM system to summarise the local tumour (T), nodal (N) and metastatic (M) extent, supplemented by PET-CT to detect occult nodal or distant disease and by brain imaging where indicated. Finally, before any operation is offered, the patient's fitness for surgery is assessed — particularly lung function (because resecting lung must leave enough functioning lung behind) and cardiac and general status. Only when histology, stage and fitness are all known can a sound management decision be made.
Provided image
- Chest X-ray first: mass, collapse, effusion, hilar change.
- Contrast CT chest + upper abdomen: tumour, mediastinal nodes, liver/adrenal metastases.
- Tissue diagnosis: bronchoscopy (central) or CT-guided needle biopsy (peripheral) → SCLC vs NSCLC + molecular testing.
- Stage by TNM + PET-CT (± brain imaging); then assess fitness for surgery (lung function, cardiac status).