Page 4 of 14
SU26.3 | Mediastinal Diseases — SDL Guide
Learning Objectives
- Describe how mediastinal disease presents, from an incidental chest X-ray finding to compressive and systemic features (SU26.3).
- Classify mediastinal masses by compartment and recall the characteristic pathology of the anterior (the four T's), middle and posterior mediastinum (SU26.3).
- Outline the principles of investigation and management of mediastinal disease, including superior vena cava obstruction (SU26.3).
INSTRUCTIONS
The mediastinum is the central compartment of the chest, packed with the great vessels, the heart, the trachea and oesophagus, lymph nodes, the thymus and nerves — so a mass here can come from any of those structures and can squeeze the others. The clinically powerful idea, which this module is built around, is that the COMPARTMENT in which a mass sits predicts what it is likely to be. Learn the anterior, middle and posterior compartments and their characteristic pathologies — especially the four T's of the anterior mediastinum — and you can reason from a chest X-ray to a sensible differential and a plan. Keep the depth at 'knows': you are learning the clinical features and principles of management, not operative technique.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 40-year-old woman attends with months of drooping eyelids and double vision that get worse as the day goes on, and weakness when she chews. A routine chest X-ray, taken because she also felt breathless, shows a mass sitting behind the upper sternum. Down the corridor, a 58-year-old smoker has come in alarmed: his face and neck have become puffy and congested, the veins on his neck stand out and do not pulsate, and he feels worse when he bends forward. Both of these very different clinical pictures lead to the same central space in the chest — the mediastinum — and both can be explained by a mass in a particular part of it. The skill you are about to build is reading the location of a mediastinal mass and reasoning from it to the likely diagnosis.
WHY THIS MATTERS
Mediastinal masses are not rare, and they range from entirely benign cysts to aggressive malignancies, so getting the reasoning right matters. Because the mediastinum holds vital structures within millimetres of one another, a mass here can be silent on a routine film or can threaten the airway and the great veins. As a clinician you will most often encounter the mediastinum as an unexpected widening on a chest X-ray, and your value lies in knowing what to think next: which compartment is it in, what does that compartment characteristically harbour, and is there compression that needs urgent attention? Recognising a thymoma behind a story of fatigable weakness, or superior vena cava obstruction behind a swollen plethoric face, turns a vague finding into a directed work-up. This compartment-based thinking is also a favourite of examiners precisely because it rewards reasoning over rote.
RECALL
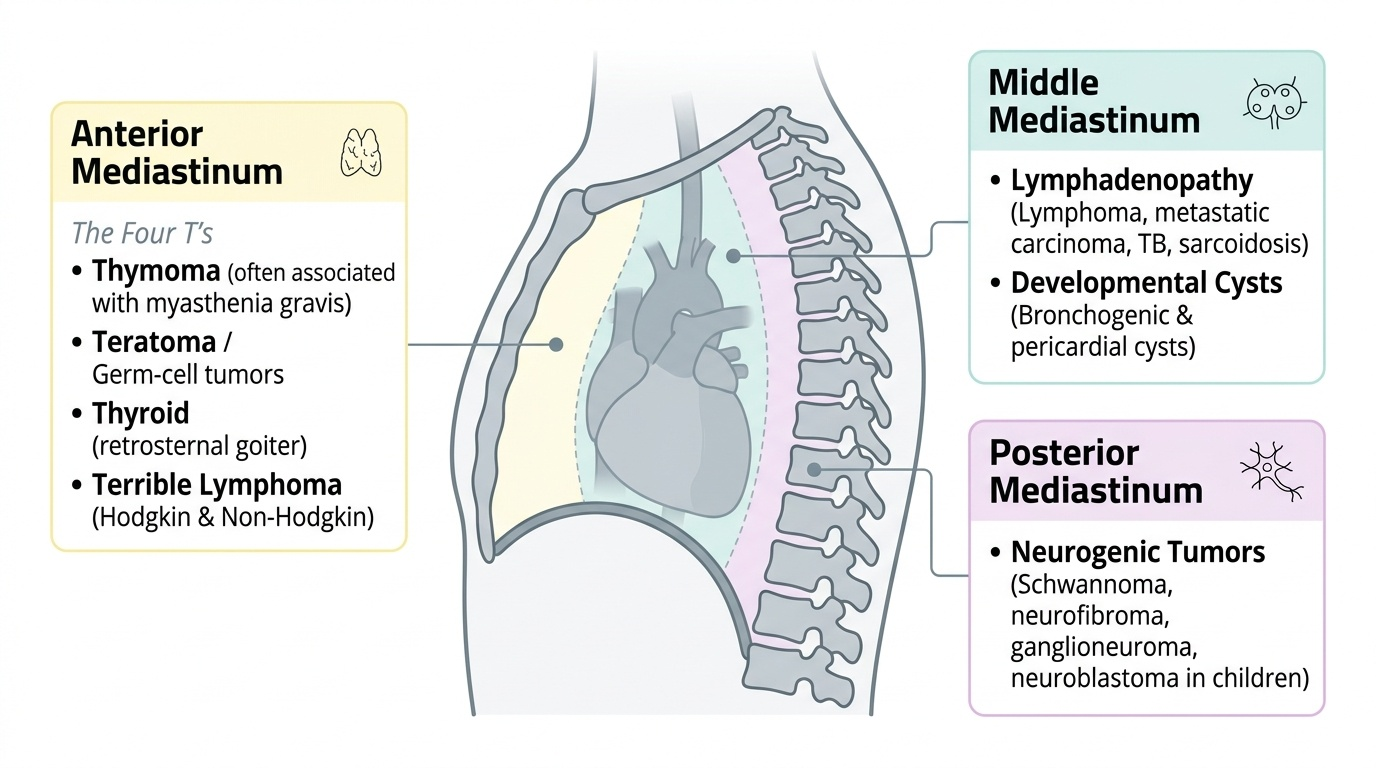
Recall the anatomy this topic rests on. The mediastinum is the space between the two pleural cavities, bounded in front by the sternum and behind by the vertebral column, and it is divided into compartments. For clinical purposes it is simplest to think of three: an anterior compartment (in front of the heart and great vessels, containing the thymus, fat and lymph nodes), a middle compartment (the heart, pericardium, great vessels, trachea and main bronchi, and many lymph nodes), and a posterior compartment (behind the heart, containing the oesophagus, descending aorta, and the sympathetic chain and spinal nerve roots). Recall too that myasthenia gravis is an autoimmune disease in which antibodies against the acetylcholine receptor cause fatigable muscle weakness — a fact that will explain one of the four T's. Holding the compartments and their contents in mind is the key to the whole module, because the contents of each compartment are exactly what its masses arise from.
The Patient with a Mediastinal Mass
Mediastinal disease presents in three broad ways, and the same mass may show one, two or all of them. First, it may be asymptomatic and incidental, discovered as a widened mediastinum or a discrete shadow on a chest X-ray or computed tomography scan requested for another reason — many benign masses, particularly in adults, are found this way. Second, it may produce local compressive symptoms as the mass pushes on the structures crowded around it: pressure on the trachea or bronchi causes cough, breathlessness or stridor; pressure on the oesophagus causes dysphagia; pressure on the recurrent laryngeal nerve causes hoarseness; and pressure on or invasion of the superior vena cava causes superior vena cava obstruction, with a swollen, plethoric face and neck, distended non-pulsatile neck veins and dilated collateral veins over the chest wall. Third, it may cause systemic or syndromic features that point to a specific tumour — most famously the fatigable weakness, ptosis and diplopia of myasthenia gravis accompanying a thymoma, but also the constitutional 'B' symptoms (fever, night sweats, weight loss) of lymphoma, or hormone- and marker-related effects of germ-cell tumours. Taking a history that screens for all three patterns, and noting the patient's age, immediately narrows the field before any imaging.
- Incidental: widened mediastinum or discrete mass on imaging done for another reason.
- Compressive: cough/stridor (airway), dysphagia (oesophagus), hoarseness (recurrent laryngeal nerve), superior vena cava obstruction.
- Systemic/syndromic: myasthenia gravis (thymoma), B symptoms (lymphoma), tumour-marker effects (germ-cell tumours).
Mediastinal Compartments and Their Characteristic Pathology
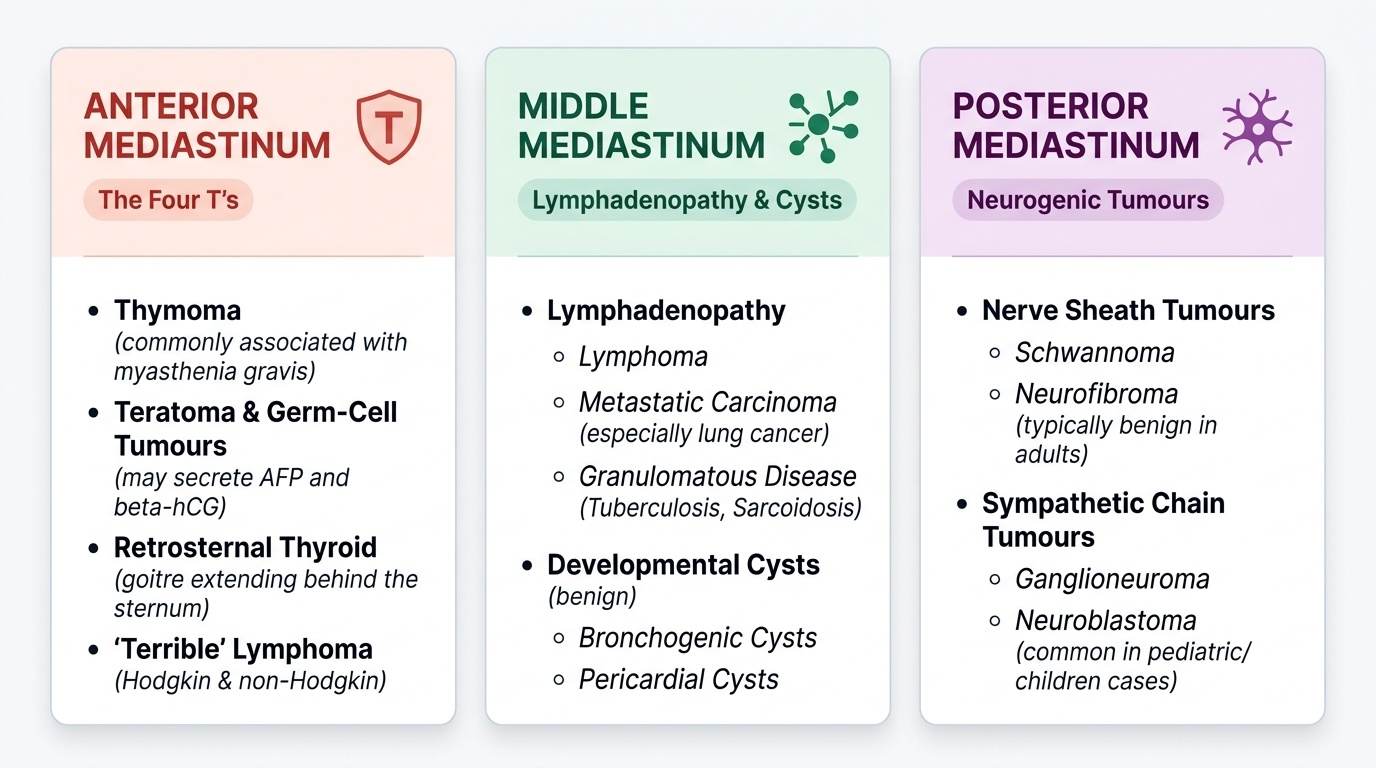
The single most useful concept in mediastinal disease is that the compartment in which a mass lies predicts its likely pathology, because each compartment's masses arise from the structures it contains. The anterior mediastinum is classically remembered by the four T's: Thymoma (a tumour of the thymus, the commonest primary anterior mediastinal tumour in adults, importantly associated with myasthenia gravis); Teratoma and other germ-cell tumours (which may secrete markers such as alpha-fetoprotein and beta-hCG); retrosternal extension of the Thyroid (a goitre that has descended behind the sternum); and 'Terrible' lymphoma (Hodgkin and non-Hodgkin lymphoma, which also frequently involves the anterior and middle mediastinum). The middle mediastinum characteristically harbours lymphadenopathy — from lymphoma, metastatic carcinoma (especially lung), or granulomatous disease such as tuberculosis and sarcoidosis — and developmental cysts such as bronchogenic and pericardial cysts, which are benign. The posterior mediastinum is the home of neurogenic tumours arising from the nerves and sympathetic chain that run there: schwannoma and neurofibroma from nerve sheaths, ganglioneuroma, and in children neuroblastoma; most are benign in adults. A mass that compresses the superior vena cava — usually an anterior or middle mediastinal malignancy such as lymphoma or, in smokers, lung cancer — produces superior vena cava obstruction, an important mechanical complication to recognise.
Provided image
Provided image
| Compartment | Characteristic masses |
|---|---|
| Anterior | The four T's: Thymoma (± myasthenia gravis), Teratoma/germ-cell tumour, retrosternal Thyroid, 'Terrible' lymphoma |
| Middle | Lymphadenopathy (lymphoma, metastatic, TB/sarcoid); bronchogenic and pericardial cysts |
| Posterior | Neurogenic tumours: schwannoma, neurofibroma, ganglioneuroma, neuroblastoma (children) |
SELF-CHECK
A patient with an anterior mediastinal mass also has fatigable muscle weakness, drooping eyelids and double vision. Which mass is most likely, and which 'T' of the anterior mediastinum does it represent?
A. A neurogenic tumour — but these are posterior, not anterior
B. A thymoma — one of the four T's, associated with myasthenia gravis
C. A bronchogenic cyst — a benign middle mediastinal lesion
D. A retrosternal thyroid — which causes hyperthyroidism, not weakness
Reveal Answer
Answer: B. A thymoma — one of the four T's, associated with myasthenia gravis
Fatigable weakness with ptosis and diplopia is myasthenia gravis, classically associated with a thymoma — the first of the anterior mediastinum's four T's (Thymoma, Teratoma/germ-cell, retrosternal Thyroid, 'Terrible' lymphoma). Neurogenic tumours are POSTERIOR; bronchogenic cysts are middle and benign; retrosternal thyroid does not cause fatigable weakness.
Investigating a Mediastinal Mass
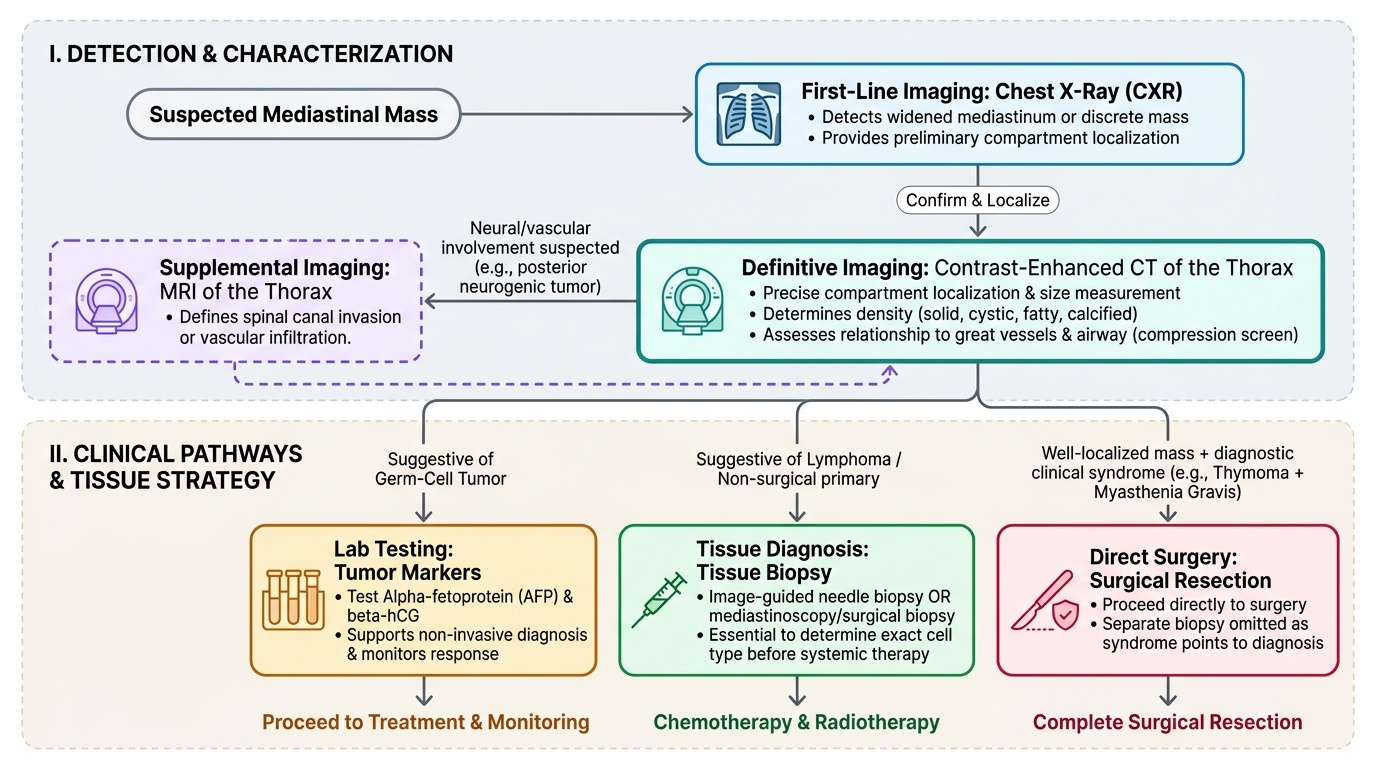
Investigation of a mediastinal mass moves logically from confirming and localising the mass, to characterising it, to obtaining a tissue diagnosis where it changes management. The first-line imaging is the chest X-ray, which may reveal a widened mediastinum or a discrete mass and gives a rough idea of its compartment. The definitive cross-sectional test is contrast-enhanced computed tomography (CT) of the thorax, which localises the mass precisely to a compartment, shows its size, density (solid, cystic, fatty or calcified) and its relationship to the great vessels and airway, and screens for compression; magnetic resonance imaging is added where neural or vascular involvement (for example a posterior neurogenic tumour invading the spinal canal) must be defined. Tumour markers are requested when a germ-cell tumour is suspected — alpha-fetoprotein and beta-hCG are raised in many malignant germ-cell tumours and can support the diagnosis and monitor treatment. Where the imaging suggests a tumour whose treatment is not primarily surgical — above all lymphoma, which is treated with chemotherapy and radiotherapy — a tissue diagnosis is obtained by image-guided needle biopsy or by mediastinoscopy/surgical biopsy, because giving the right treatment depends on knowing the cell type. A well-localised mass with a syndrome that already points to the diagnosis (such as a thymoma with myasthenia gravis) may proceed to surgery without separate biopsy.
Provided image
- Chest X-ray first: widened mediastinum / discrete mass, rough compartment.
- Contrast CT thorax: precise compartment, size, density, vessel/airway relations; MRI for neural/vascular involvement.
- Tumour markers (AFP, beta-hCG) when a germ-cell tumour is suspected.
- Tissue biopsy (needle / mediastinoscopy) when treatment is non-surgical, especially suspected lymphoma.