Page 1 of 14
SU26.1 | Surgery for Heart Disease — SDL Guide
Learning Objectives
- Outline the role of surgery in coronary (ischaemic) heart disease, including the indications for coronary artery bypass grafting (SU26.1).
- Outline the role of surgery in valvular heart disease, including valve repair versus replacement and the choice between mechanical and bioprosthetic valves (SU26.1).
- Outline the role of surgery in congenital heart disease, distinguishing acyanotic left-to-right shunts from cyanotic lesions and the principle of cardiopulmonary bypass (SU26.1).
INSTRUCTIONS
Heart surgery looks formidable, but a final-year student does not need to perform it — you need to understand WHEN it helps and WHAT it achieves, so you can counsel a patient and recognise the surgical referral. This module takes the three problems the competency names — blocked coronary arteries, diseased valves, and holes or malformations present from birth — and explains, at the level of principles rather than operative detail, why surgery is offered, what cardiopulmonary bypass makes possible, and how the surgeon chooses between repairing and replacing, and between a mechanical and a tissue valve. Keep the depth at 'knows': the goal is sound clinical reasoning, not a surgical manual.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients sit in a cardiac clinic on the same morning. The first is a 62-year-old man with crushing central chest pain on walking; his angiogram shows that all three of his coronary arteries are severely narrowed. The second is a 55-year-old woman who is breathless climbing stairs; her aortic valve has become so tight and calcified that her heart is straining to push blood past it. The third is a baby boy who turns blue when he cries, born with a heart that was never plumbed correctly. None of these problems will be cured by tablets alone — each may need a surgeon to restore blood flow, replace a worn-out valve, or close a defect. Understanding which patient needs which operation, and why, is the heart of this topic.
WHY THIS MATTERS
Heart disease is among the commonest causes of death worldwide, and cardiac surgery turns several otherwise progressive or fatal conditions into treatable ones. As a doctor you will not operate, but you will be the person who recognises the patient who should be referred, explains the proposed operation in plain language, and follows the patient afterwards — for example checking the anticoagulation of someone with a mechanical valve, or counselling the parents of a child with a congenital defect. Knowing the role of surgery also keeps your medical management honest: you offer angioplasty or drugs where they suffice and refer for bypass or valve surgery where the evidence and anatomy demand it. Even a knows-level grasp of cardiopulmonary bypass demystifies how a beating organ can be safely stopped, opened and repaired.
RECALL
Recall a few foundations before we build on them. From anatomy and physiology: the coronary arteries (right, and the left main dividing into the left anterior descending and circumflex) supply the heart muscle itself, so a blockage starves the myocardium and causes angina or infarction. The four cardiac valves keep blood moving one way through the cardiac cycle, so a stenosed (narrowed) valve obstructs forward flow while a regurgitant (leaky) valve lets blood flow backwards, both overloading the chambers. From basic physiology of shunts: in a normal heart no oxygenated and deoxygenated blood mix; an abnormal communication produces a left-to-right shunt (oxygenated blood recirculates through the lungs — the child is pink/acyanotic) or, if pressures reverse or the anatomy is severe, a right-to-left shunt (deoxygenated blood reaches the body — the child is blue/cyanotic). Hold on to these ideas — every operation in this module corrects one of them.
The Patient Referred for Cardiac Surgery
Patients reach the cardiac surgeon along three recognisable routes that mirror the three disease groups. The first is ischaemic (coronary) heart disease: the typical patient is middle-aged or older with risk factors such as smoking, diabetes, hypertension and hyperlipidaemia, who presents with angina — central chest pain or tightness brought on by exertion and relieved by rest — or who has survived a myocardial infarction. When symptoms persist despite medication, or when investigation reveals disease in the left main stem or in all three coronary arteries, the question of surgical revascularisation arises. The second route is valvular heart disease: the patient complains of exertional breathlessness, fatigue, palpitations, chest pain or syncope, and a murmur is heard on examination; aortic stenosis classically causes angina, syncope and breathlessness, while mitral or aortic regurgitation present with progressive breathlessness as the overloaded ventricle fails. The third route is congenital heart disease, recognised in infancy or childhood: an acyanotic child may have a murmur, recurrent chest infections or failure to thrive from a left-to-right shunt, whereas a cyanotic child turns blue, especially on crying or feeding. Recognising which of these three stories a patient tells is the first step toward the right operation.
- Ischaemic: exertional angina or post-infarction; refer when medical therapy fails or anatomy is high-risk (left main / triple-vessel).
- Valvular: breathlessness, fatigue, syncope, murmur; stenosis obstructs, regurgitation leaks.
- Congenital: acyanotic (murmur, failure to thrive, chest infections) vs cyanotic (blue spells).
Surgical Basis: Why and How the Heart Is Operated On
Surgery is offered when a mechanical problem in the heart can be physically corrected and when doing so improves symptoms or survival more than medicine alone. In coronary disease the problem is a fixed obstruction to blood flow in the coronary arteries; surgery bypasses the blockage with a new conduit so oxygenated blood again reaches the starved muscle. In valvular disease the problem is a valve that is either too tight (stenosis) or too leaky (regurgitation), chronically overloading and eventually failing the ventricle; surgery repairs or replaces the valve before that damage becomes irreversible. In congenital disease the problem is an abnormal communication or malformation that mixes blood or obstructs flow; surgery closes the defect or reconstructs the outflow. Most of these corrections require the surgeon to open the heart while it is still and bloodless, which is impossible in a continuously beating, blood-filled organ. The enabling technology is the cardiopulmonary bypass machine (the heart-lung machine): deoxygenated blood is drained from the great veins into the machine, passed through an oxygenator that adds oxygen and removes carbon dioxide (taking over the lung's job) and a heat exchanger that controls temperature, then pumped back into the aorta to perfuse the body — taking over the heart's pumping job. With circulation thus maintained by the machine, the heart is isolated with an aortic cross-clamp and stopped using cardioplegia (a potassium-rich solution), giving the surgeon a still, bloodless field to work in.
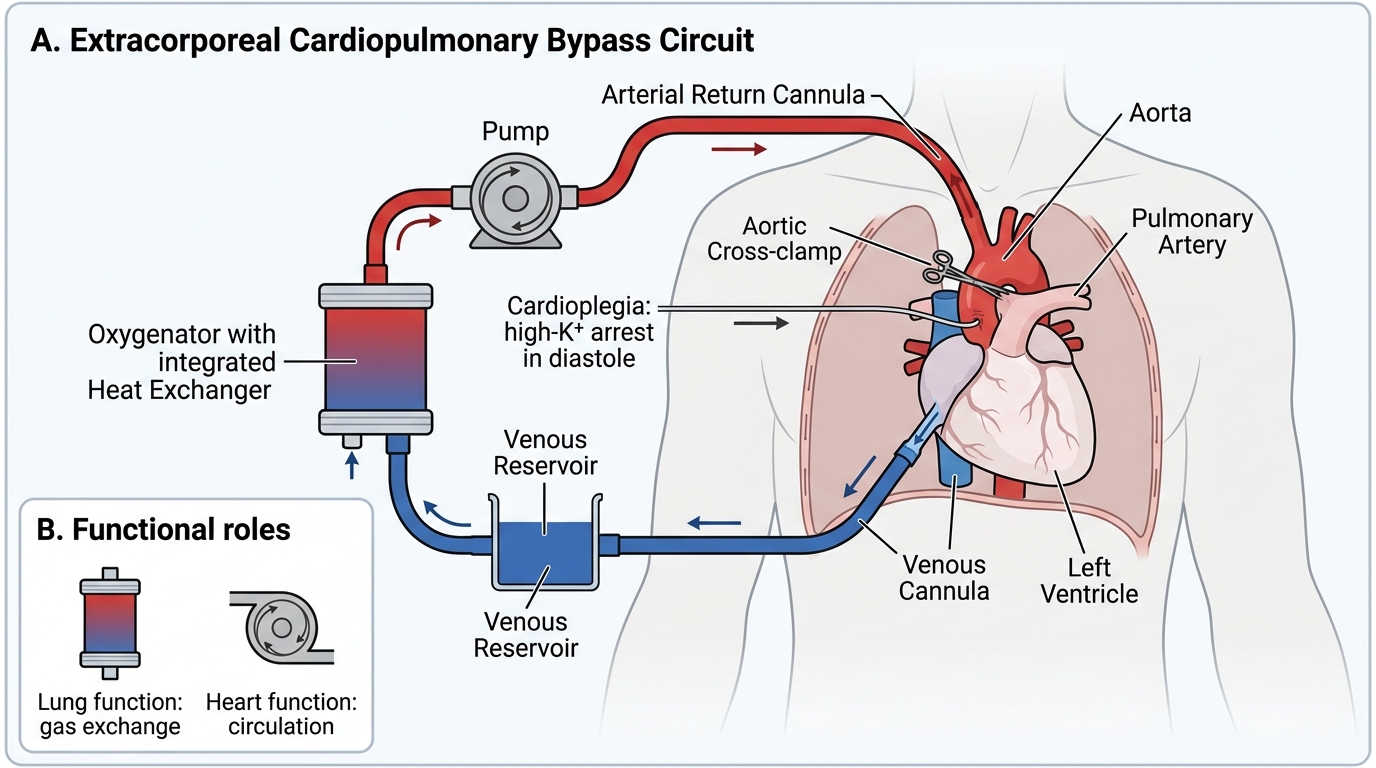
Cardiopulmonary Bypass Circuit
- Cardiopulmonary bypass = oxygenator (lung function) + pump (heart function), allowing the heart to be safely stopped.
- Cardioplegia (high-potassium solution) arrests the heart in diastole for a still operative field.
- Not every operation needs bypass: a patent ductus and some bypass grafts can be done off-pump or without opening the heart.
SELF-CHECK
What is the primary purpose of the cardiopulmonary bypass (heart-lung) machine during open-heart surgery?
A. To permanently replace the function of a failing heart
B. To temporarily take over the pumping and gas-exchange functions of the heart and lungs so the heart can be stopped and operated on
C. To deliver anticoagulation to prevent valve thrombosis
D. To measure coronary artery blood flow during the operation
Reveal Answer
Answer: B. To temporarily take over the pumping and gas-exchange functions of the heart and lungs so the heart can be stopped and operated on
Cardiopulmonary bypass temporarily takes over both the heart's pumping and the lungs' gas-exchange functions, oxygenating the blood and circulating it to the body while the heart is stopped (with cardioplegia) and isolated by an aortic cross-clamp, giving the surgeon a still, bloodless field. It is a temporary support, not a permanent replacement, and is removed once the repair is complete.
Assessment and Investigation Before Cardiac Surgery
Before any cardiac operation the patient is assessed both to confirm the lesion and to judge whether they will survive and benefit from surgery. The cornerstone investigations differ by disease but follow a logical order. For coronary disease, coronary angiography is the definitive test: a catheter injects contrast into the coronary arteries to map exactly which vessels are narrowed and how severely, and this anatomy decides between medical therapy, percutaneous coronary intervention (angioplasty and stenting) and surgical bypass — broadly, disease of the left main stem or of all three vessels, especially in diabetics, favours bypass surgery. For valvular disease, echocardiography is the key test, showing which valve is affected, whether it is stenotic or regurgitant, how severe the lesion is, and how well the ventricle is still contracting (the ejection fraction). For congenital disease, echocardiography again defines the anatomy of the defect and the direction and size of any shunt, supplemented where needed by cross-sectional imaging or catheterisation. Across all three, the patient also has a baseline electrocardiogram and chest X-ray, blood tests, and an assessment of general fitness — lung function, kidney function and other comorbidity — because cardiopulmonary bypass and a sternotomy are major physiological insults. This pre-operative work-up is what converts a diagnosis into a sound, individualised surgical decision.
- Coronary disease → coronary angiography maps the vessels and guides medicine vs PCI vs bypass.
- Valvular disease → echocardiography defines the valve lesion, its severity and ventricular function.
- Congenital disease → echocardiography defines the defect and shunt direction/size.
- All: ECG, chest X-ray, bloods and a general fitness/comorbidity assessment before bypass.