Page 5 of 11
SU2.3 | Shock Prognosis Counselling — SDL Guide (Part 2)
Applying the Framework: Worked Conversations
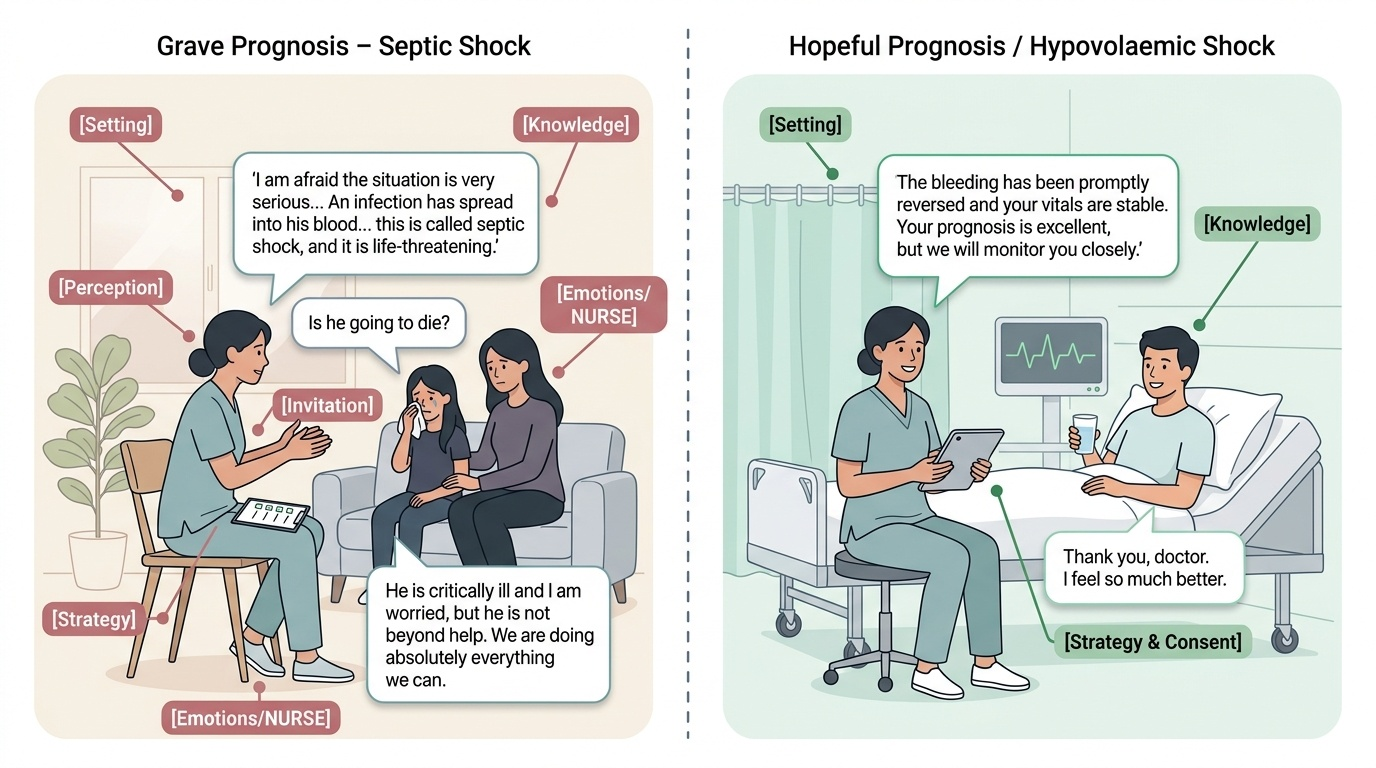
Principles and frameworks come alive only in worked practice, so consider two contrasting conversations that a final-year student should be able to conduct. In the first, you must inform the wife and daughter of the man in septic shock from the hook, whose prognosis is guarded. You take them to a quiet room, sit down (Setting), and ask what they understand (Perception); they know only that he is 'very unwell'. You ask how much they want to know (Invitation) and give a warning shot — 'I am afraid the situation is very serious' — before explaining in plain words (Knowledge): 'An infection has spread into his blood and dropped his blood pressure so low that his kidneys and other organs are struggling — this is called septic shock, and it is life-threatening. We are giving strong antibiotics, fluids and medicines to support his blood pressure, and he is in the intensive care unit.' When the daughter begins to cry you pause, then respond with empathy (Emotions/NURSE): 'I can see how devastating this is — anyone would feel this way. We are doing absolutely everything we can.' When she asks directly, 'Is he going to die?', you answer honestly but kindly: 'He is critically ill and I am worried, but he is not beyond help; the next twenty-four hours will tell us a great deal, and I promise to keep you informed.' You close with a plan and a contact (Strategy). In the second, contrasting conversation, you reassure and consent an alert young man whose hypovolaemic shock from a bleed has been promptly reversed; here the same framework is used but the prognosis is genuinely good, so the tone is calm and reassuring while still honest about what was done and what to watch for. The two scripts show the same structure flexing to fit a grave and a hopeful prognosis — that flexibility, anchored in honesty, is the skill.
Provided image
Reviewing the Conversation: What Good Looks Like
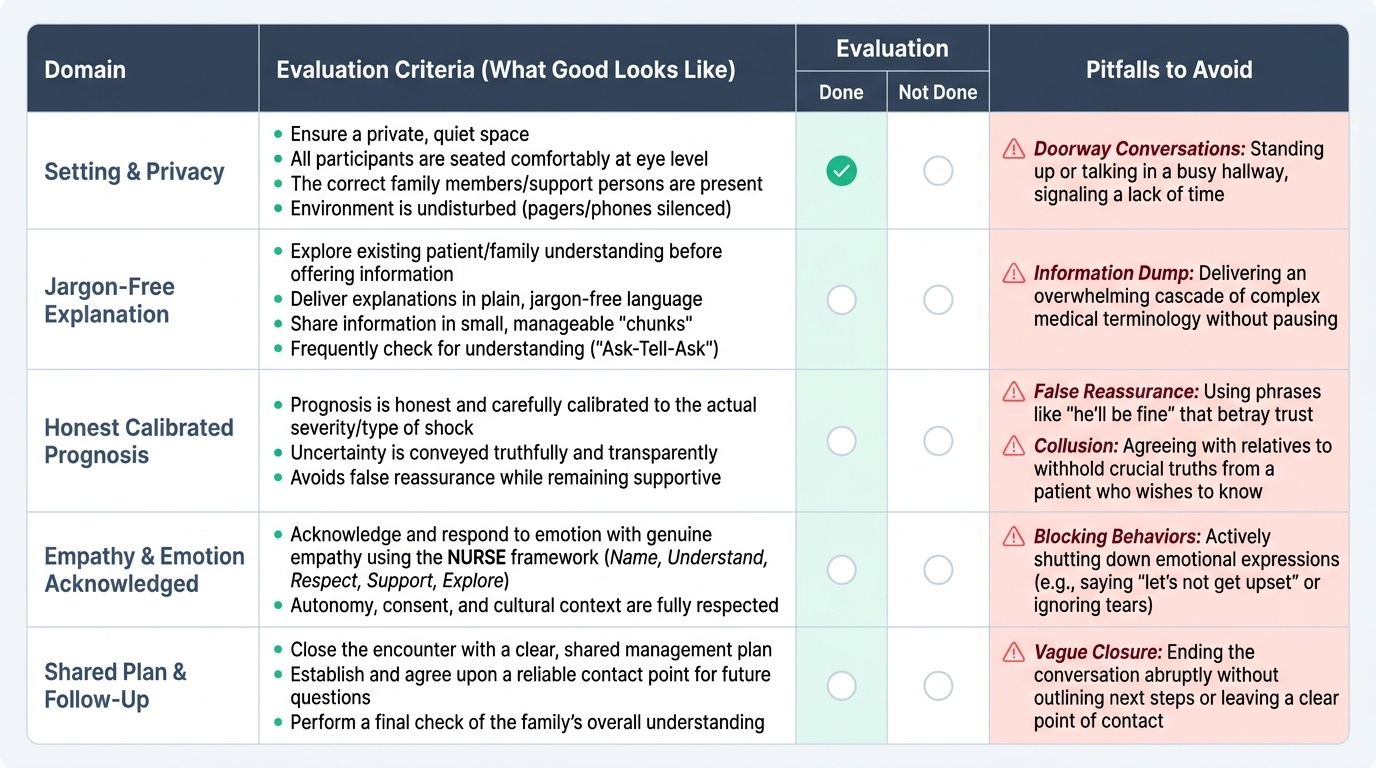
Communication is a skill, and like any skill it improves only through honest review and feedback, so the final step is learning to evaluate an encounter against a clear standard rather than by gut feeling alone. A good counselling conversation about shock can be appraised against a simple checklist: was the setting appropriate (private, seated, the right people, uninterrupted)? Was the patient's or family's existing understanding explored before information was given? Was the information delivered in plain, jargon-free language, in manageable chunks, with understanding checked? Was the prognosis honest and calibrated to the actual type and severity of the shock — neither falsely reassuring nor needlessly bleak — and was uncertainty conveyed truthfully? Was emotion acknowledged and responded to with genuine empathy rather than blocked or ignored? Were autonomy, consent and cultural context respected? And did the conversation close with a shared plan, a contact point and a check of understanding? Equally important is recognising the recurring pitfalls that a reviewer looks for: false reassurance ('he'll be fine') that betrays trust; the information dump of jargon that overwhelms; blocking behaviours that shut down emotion ('let's not get upset'); collusion with relatives to withhold the truth from a patient who wants it; and the cold, standing, doorway conversation that signals the clinician has no time. Using a rubric like this — to debrief your own simulated encounters and to receive feedback from peers and faculty — is how the 'shows-how' competency is genuinely acquired rather than merely understood.
Provided image
- Setting: private, seated, right people, undisturbed.
- Perception explored before information given.
- Plain language, chunked, understanding checked.
- Prognosis honest and calibrated; uncertainty conveyed truthfully.
- Emotion acknowledged with empathy (NURSE).
- Autonomy, consent, culture respected; shared plan + contact agreed.
- Pitfalls to avoid: false reassurance, information dump, blocking, collusion.
CLINICAL PEARL
When a family member asks the question you dread — 'Is he going to die?' — do not deflect it and do not answer with false comfort. Acknowledge the courage of the question, answer honestly in a way calibrated to the real prognosis, and protect a realistic measure of hope: 'That is exactly the right question to ask. He is critically ill and I am genuinely worried, but he is not beyond help and we are doing everything we can — the next day will tell us much more.' Honesty and hope are not opposites; the skill is to hold both, and a few seconds of shared silence after the answer is more comforting than any extra words.
Check Your Understanding
Bring the threads together by reasoning back through the two worked conversations. For the family of the man in septic shock, satisfy yourself that you could run the full SPIKES sequence — settle them privately, find out what they know, ask how much they want told, give a warning shot and then a plain-language explanation of septic shock and its treatment, respond to their distress with the NURSE empathic stems, answer the 'will he die?' question with calibrated honesty, and close with a clear plan and a point of contact. For the recovering young man with reversed hypovolaemic shock, satisfy yourself that you could use the same structure to reassure honestly, explain what happened and what to watch for, and obtain his informed consent and understanding. Now self-test the competency this module covers. First, can you state why honest, empathic communication is itself a core clinical skill in shock, and why SU2.3 is examined at the 'shows-how' level? Second, can you name and apply the SPIKES steps and the NURSE empathic responses, and explain how to calibrate a prognosis honestly to the type and severity of shock without removing hope? Third, can you evaluate a counselling encounter against a rubric and name the common pitfalls — false reassurance, the information dump, blocking and collusion — that you must avoid? The questions that follow check exactly these links.
SELF-CHECK
In the SPIKES protocol, what is the purpose of the 'P — Perception' step before giving any information about the patient's shock?
A. To obtain written consent for the discussion
B. To find out what the patient or family already understands so the explanation can correct misunderstandings and be pitched correctly
C. To deliver the prognosis as early as possible
D. To document the conversation in the notes
Reveal Answer
Answer: B. To find out what the patient or family already understands so the explanation can correct misunderstandings and be pitched correctly
‘P — Perception’ means assessing what the patient or family already knows ('What have you been told so far?') BEFORE giving information, so you can correct misunderstandings and pitch your explanation at the right level. Invitation (asking how much they want to know) and Knowledge (giving the information) come after. It is a 'before you tell, ask' step, not consent, prognosis-first delivery, or documentation.