Page 10 of 20
SU27.5-6 | Lower Limb Venous Disorders — SDL Guide
Learning Objectives
- Describe the applied anatomy of the venous system of the lower limb — the superficial and deep systems, perforators, valves and the calf muscle pump (SU27.5).
- Describe the pathophysiology, clinical features, investigations and principles of management of deep vein thrombosis and varicose veins (SU27.6).
INSTRUCTIONS
Blood returning from the leg flows uphill against gravity, and it depends on competent valves and the calf muscle pump to do so. When the superficial valves fail, blood pools and the veins dilate into varicose veins; when a deep vein clots, the leg swells acutely and a fragment may break off to the lungs. These two disorders — one chronic and visible, one acute and dangerous — are the everyday venous pathology of surgery. This module first lays down the applied venous anatomy that explains both, then works through the pathophysiology, clinical features, bedside tests and duplex investigation, and the principles of management: compression and ablation for varicose veins, and prompt anticoagulation for deep vein thrombosis with its threat of pulmonary embolism.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old shopkeeper who stands all day complains of aching, heavy legs by evening and unsightly ropy veins bulging on the inside of her calf; lately the skin above her ankle has darkened and itched, and a shallow ulcer has appeared just above the bone. In the next bay, a 60-year-old man who flew home last week and has been in bed since a hip operation has a left calf that is suddenly swollen, warm and tender, and he has just become breathless. Both problems live in the veins of the leg, but they could not be more different: one is a slow, chronic failure of valves that you will manage over months, the other an acute clot that may already be showering emboli into the lungs and demands treatment today. Understanding the venous anatomy that links them, and telling the chronic from the emergency, is the work of this topic.
WHY THIS MATTERS
Venous disease of the leg is extremely common and spans the trivial to the lethal. Varicose veins and chronic venous insufficiency affect a large fraction of adults, cause aching, swelling, skin damage and venous ulcers that are slow to heal and costly to society, and are a frequent surgical referral. Deep vein thrombosis, at the other extreme, is a leading preventable cause of in-hospital death because of its complication, pulmonary embolism — which is exactly why thromboprophylaxis is built into every surgical admission. As a clinician you will be expected to examine a leg for varicose veins and venous skin changes, recognise and risk-assess a possible DVT, and know the one rule that prevents a catastrophic error — never to apply tight compression to a leg without first excluding arterial disease. For a final-year student, the applied venous anatomy and the bedside discrimination of venous from arterial disease are core, examinable knowledge.
RECALL
Recall the anatomy and physiology this builds on. From AN: the leg has a deep venous system (running with the arteries) and a superficial system in the subcutaneous fat — the great (long) saphenous vein on the medial side and the small (short) saphenous vein at the back of the calf — joined to the deep veins by perforating veins. From PY: venous return from the leg works against gravity and is driven by the calf muscle pump squeezing the deep veins during walking, while one-way venous valves ensure blood flows only upward (superficial to deep, and toward the heart) and does not reflux. Hold on to this single idea: every lower-limb venous disorder is a failure of this system — valvular incompetence lets blood reflux and pool (varicose veins and venous insufficiency), whereas a thrombus blocks the deep veins (DVT). The competent valve and the working calf pump are what keep the leg healthy, and their failure explains everything that follows.
Aching Legs, Visible Veins and the Swollen Calf
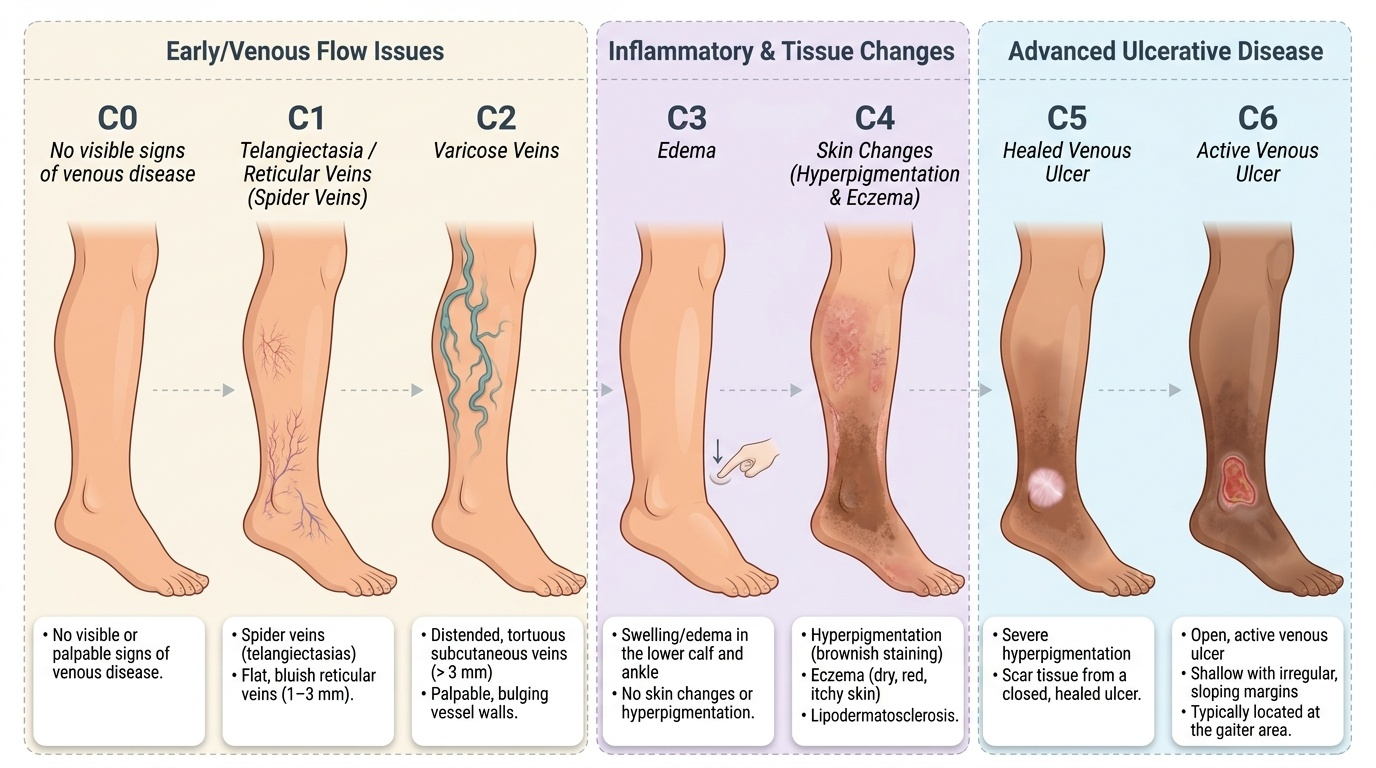
Lower-limb venous disease presents in two clinically distinct ways, and separating them is the first task. Chronic venous disease from valvular incompetence presents insidiously: dilated, tortuous superficial veins (varicose veins), aching, heaviness and itching that are worse on prolonged standing and relieved by elevation, ankle swelling, and — as venous hypertension damages the skin — pigmentation, eczema, hardening of the subcutaneous tissue (lipodermatosclerosis) and finally a venous ulcer, classically over the medial malleolus (the gaiter area). Complications also include superficial thrombophlebitis and bleeding from a thin-walled varix. By contrast, deep vein thrombosis (DVT) presents acutely: a unilateral, swollen, warm, tender calf or thigh, sometimes with dilated superficial veins and a positive (but unreliable) calf tenderness, developing over hours to days. The crucial danger of DVT is its silent extension and embolisation to the lungs — pulmonary embolism (PE) — which presents with sudden breathlessness, pleuritic chest pain, haemoptysis or collapse, so any swollen leg with new respiratory symptoms is an emergency. Ask carefully about provoking factors for DVT — recent surgery or immobility, long travel, malignancy, pregnancy or the oral contraceptive pill, and previous thrombosis — and, for chronic disease, about standing occupation, previous DVT and the duration of any ulcer.
Applied Venous Anatomy and the Pathophysiology of Venous Disease
The applied anatomy explains both diseases. The leg drains through two systems: the deep veins, enclosed by muscle and carrying most of the return, and the superficial veins in the subcutaneous tissue — the great (long) saphenous vein, which runs up the medial leg and thigh to drain into the femoral vein at the sapheno-femoral junction in the groin, and the small (short) saphenous vein, which runs up the back of the calf to drain into the popliteal vein at the sapheno-popliteal junction behind the knee. Perforating veins connect the superficial to the deep system, and one-way valves throughout ensure flow goes only from superficial to deep and upward; the calf muscle pump propels blood toward the heart on walking. Varicose veins arise when these valves become incompetent — most often a primary failure starting at the sapheno-femoral or sapheno-popliteal junction, or perforator incompetence — so blood refluxes and pools, raising venous pressure and dilating the superficial veins (secondary varicose veins follow a previous DVT or pelvic venous obstruction). Sustained venous hypertension is what produces the skin changes and ulcer of chronic venous insufficiency. Deep vein thrombosis is explained by Virchow's triad — venous stasis, endothelial (vessel-wall) injury and hypercoagulability: the three factors that, alone or together (as in surgery, immobility, trauma, malignancy or thrombophilia), promote clot formation in the deep veins, from where it can propagate proximally and embolise to the lungs. The chronic disease of the superficial system and the acute disease of the deep system thus share one anatomical stage but arise by opposite mechanisms — reflux versus thrombosis.
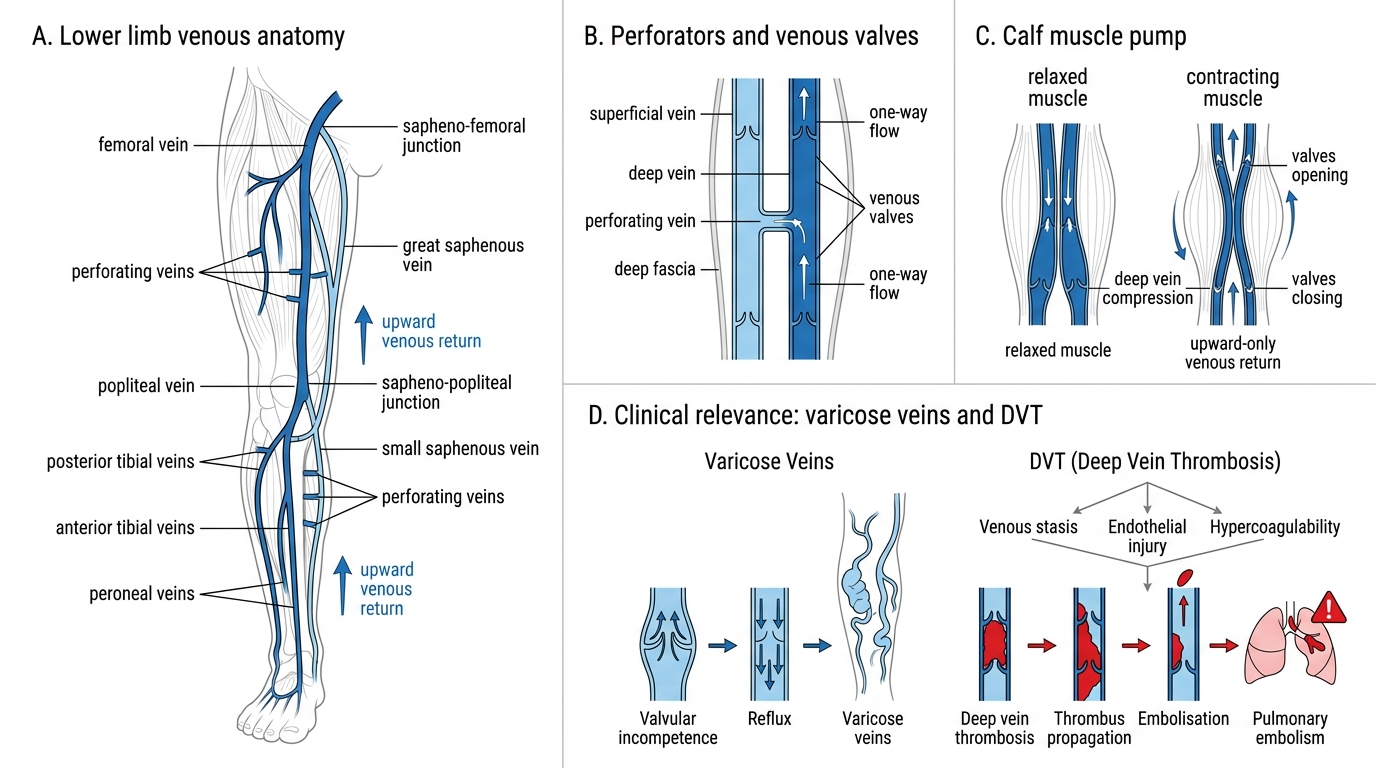
Lower Limb Venous System and Calf Muscle Pump
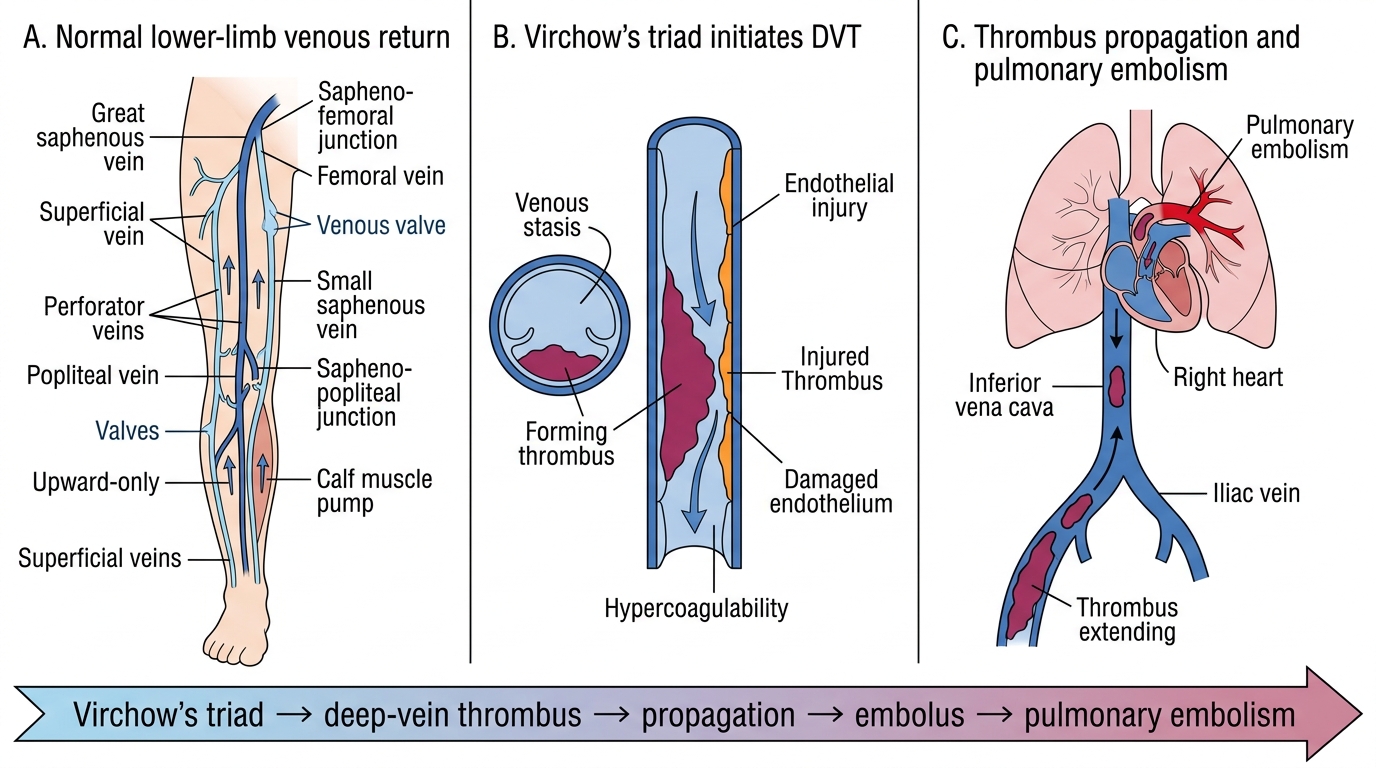
Deep Vein Thrombosis and Pulmonary Embolism Mechanism
- Superficial system: great saphenous → femoral vein at sapheno-femoral junction (groin); small saphenous → popliteal vein at sapheno-popliteal junction (behind knee).
- Deep system + perforators + valves + calf muscle pump = the upward-only return mechanism.
- Varicose veins: valvular incompetence → reflux (primary, or secondary to DVT/pelvic obstruction).
- DVT: Virchow's triad — stasis, endothelial injury, hypercoagulability → deep-vein clot → risk of PE.
SELF-CHECK
The great (long) saphenous vein drains into the deep venous system at which anatomical site, and what is the underlying defect that produces primary varicose veins?
A. The sapheno-popliteal junction; arterial reflux
B. The sapheno-femoral junction in the groin; incompetent venous valves causing reflux
C. The popliteal fossa; deep vein thrombosis
D. The femoral triangle; lymphatic obstruction
Reveal Answer
Answer: B. The sapheno-femoral junction in the groin; incompetent venous valves causing reflux
The great saphenous vein drains into the femoral vein at the sapheno-femoral junction in the groin (the small saphenous drains into the popliteal vein at the sapheno-popliteal junction behind the knee). Primary varicose veins result from incompetent venous valves — commonly at these junctions or in perforators — that allow blood to reflux and pool in the superficial veins.
Examination and Investigation
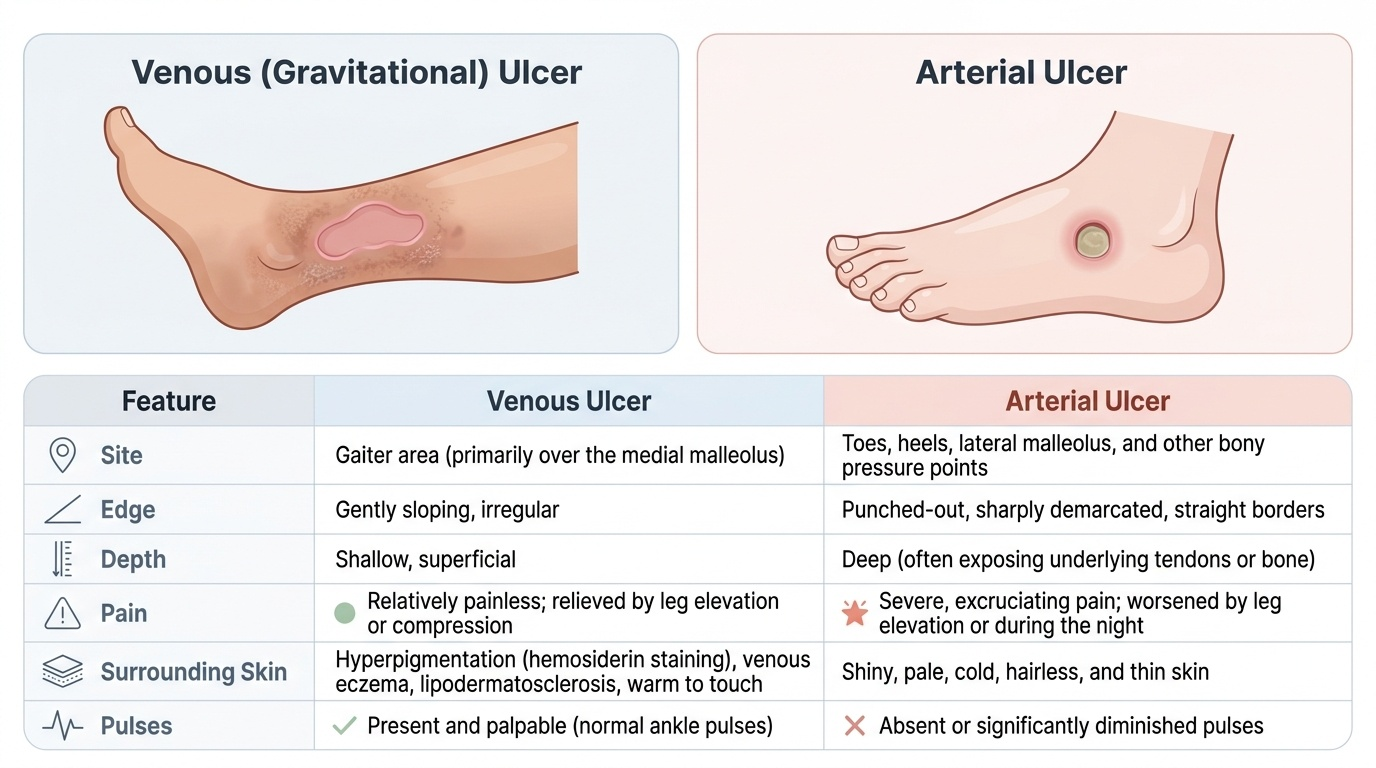
Examination of the venous system is directed by which disorder you suspect. For varicose veins, inspect the standing patient for the distribution of varicosities (great versus small saphenous territory), and for the skin changes of chronic venous insufficiency — pigmentation, venous eczema, lipodermatosclerosis and ulceration at the medial malleolus. The venous (gravitational) ulcer is characteristically shallow with sloping edges, over the gaiter area, relatively painless, with surrounding skin changes and palpable foot pulses — the opposite of the painful, punched-out arterial ulcer over pressure points or toes with absent pulses. Classic bedside tests localise the incompetence: the cough impulse and tap test at the sapheno-femoral junction, and the Trendelenburg test / tourniquet test (elevate to empty the veins, apply a tourniquet at successive levels, then stand the patient — controlled filling indicates the level of incompetent valves). For DVT, examine for a unilateral swollen, warm, tender calf and measure the calf circumference. The investigation of both now centres on duplex ultrasound, which is the gold standard: it maps the sites of reflux and junctional/perforator incompetence in varicose veins, and it directly demonstrates (or excludes) thrombus in the deep veins for DVT. For suspected DVT, use the Wells score to assign clinical probability: a low-probability score with a negative D-dimer effectively excludes DVT, whereas a high-probability score (or a positive D-dimer) proceeds to compression duplex ultrasound for confirmation. Stage chronic venous disease with the CEAP classification (C0–C6). Crucially, before applying any compression therapy, always measure the ABPI to exclude significant arterial disease — compressing an ischaemic leg can cause tissue necrosis.
Provided image
Provided image
- Varicose veins: inspect distribution and skin changes; Trendelenburg/tourniquet and cough/tap tests localise incompetence.
- Venous ulcer: gaiter area (medial malleolus), shallow, sloping, relatively painless, foot pulses present (vs arterial: toes/pressure points, punched-out, painful, pulseless).
- Duplex ultrasound: gold standard — maps reflux (varicose veins) and confirms/excludes deep-vein thrombus (DVT).
- DVT pathway: Wells score → low + negative D-dimer excludes; otherwise compression duplex.
- Always check ABPI before compression; stage chronic disease by CEAP (C0–C6).