Page 1 of 17
SU28.1-2 | Hernias — SDL Guide
Learning Objectives
- Describe the pathophysiology, anatomy and clinical features of inguinal, femoral and other abdominal-wall hernias, and the continuum from a reducible to a strangulated hernia (SU28.1).
- Describe the investigations and principles of management of hernias, including open mesh and laparoscopic repair and the indications for emergency surgery (SU28.1).
- Demonstrate the correct technique to examine a patient with a hernia and identify the different types, distinguishing indirect from direct inguinal and inguinal from femoral hernias (SU28.2).
INSTRUCTIONS
A hernia — the protrusion of a viscus or part of a viscus through a weakness in the wall that contains it — is one of the commonest conditions in general surgery and one of the commonest operations a surgeon performs. The clinical task is twofold: recognise the lump and classify it correctly, and recognise the dangerous moment when a hernia stops being a harmless bulge and threatens the blood supply of its contents. This module connects the surgical anatomy of the groin to a disciplined examination, an understanding of the reducible-to-strangulated continuum, and the modern principles of repair.
References
- Bailey & Love's Short Practice of Surgery, Hernias, Umbilicus and Abdominal Wall (textbook)
- SRB's Manual of Surgery, Hernia (textbook)
- Sabiston Textbook of Surgery, Hernias (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 45-year-old labourer comes to clinic with a lump in his right groin that has been there for two years. It appears when he stands or coughs and disappears when he lies down, and it does not hurt. In the next cubicle is a 70-year-old woman brought in by her family: she has a small, exquisitely tender lump just below the crease of her right groin, has been vomiting since morning, and her abdomen is becoming distended. The first lump is a nuisance that can be planned for; the second is a surgical emergency in which a loop of bowel is being slowly throttled. Both are hernias — the same basic problem of a viscus pushing through a wall — but they sit at opposite ends of a continuum, and your job is to tell, at the bedside, exactly where on that continuum a patient lies.
WHY THIS MATTERS
Hernias are extremely common, and inguinal hernia repair is among the most frequently performed general-surgical operations worldwide. Most hernias are uncomplicated and can be repaired electively, but a minority obstruct or strangulate, and a strangulated hernia is a true emergency in which delay costs bowel and occasionally life. The skill that protects your patients is the ability to examine a groin lump, decide which type of hernia it is, and judge whether it is reducible or in trouble. Getting the anatomy right also matters in theatre, because the difference between an indirect and a direct hernia, and the proximity of the femoral vessels and the inferior epigastric vessels, dictates how the repair is done and what must not be injured. For a final-year student, a groin examination is a guaranteed clinical-examination station and a skill you will use throughout your career.
RECALL
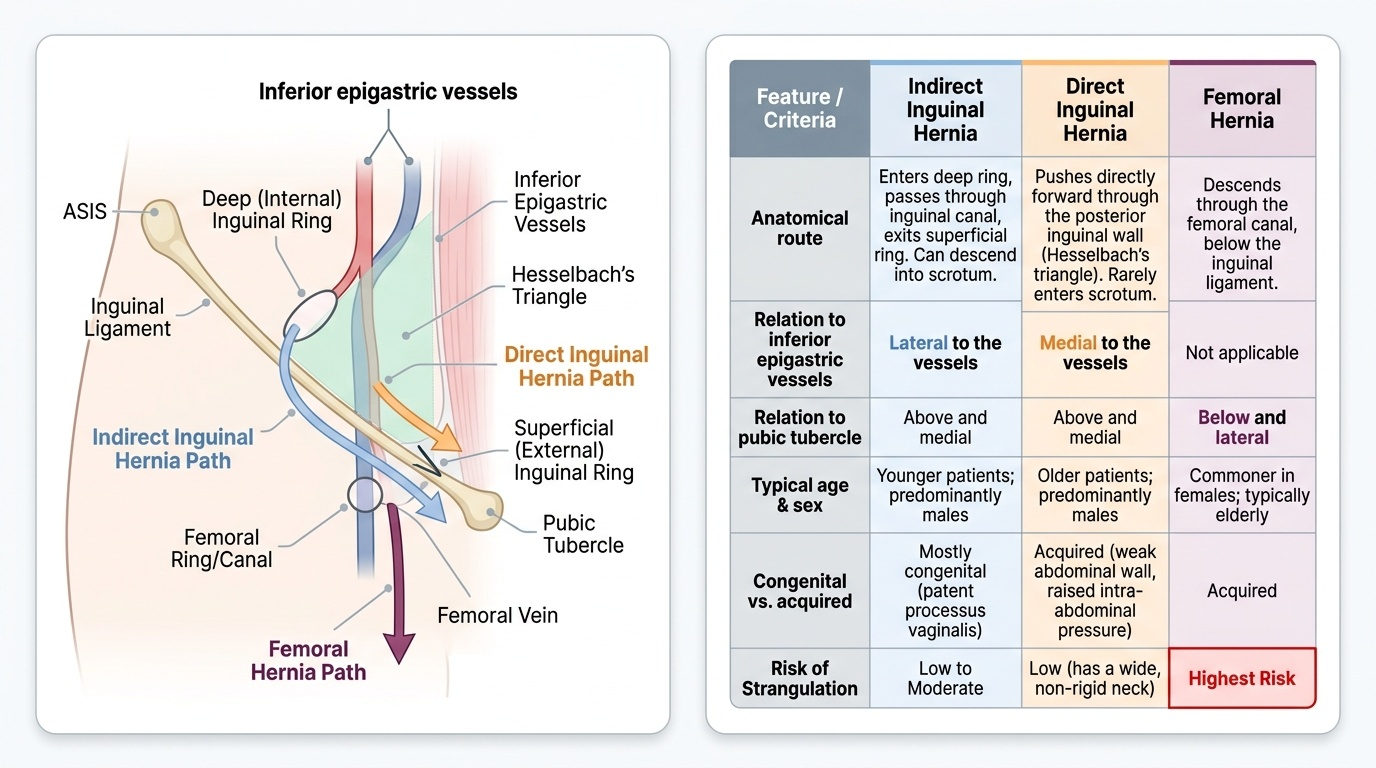
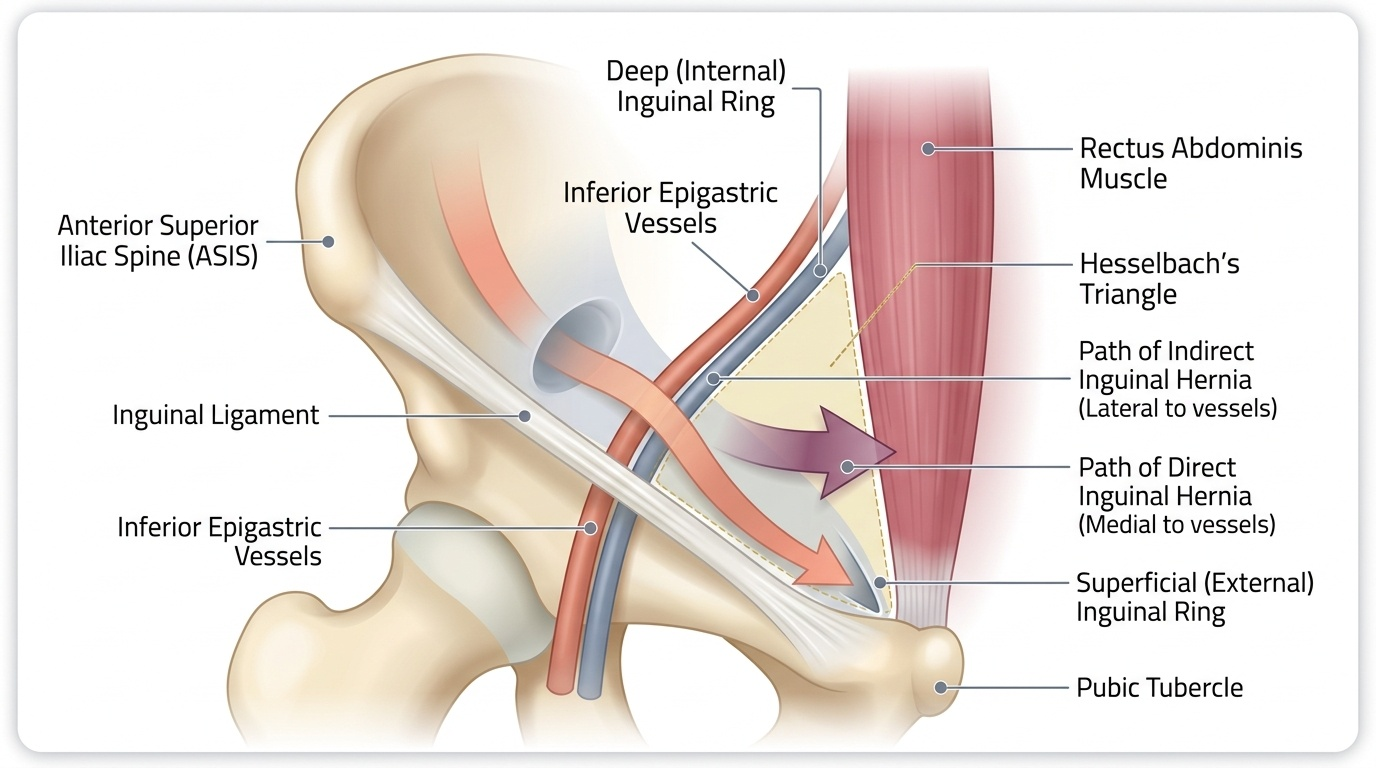
Recall the anatomy of the inguinal region before we build on it. The inguinal canal is an oblique passage in the lower anterior abdominal wall transmitting the spermatic cord in the male and the round ligament in the female; it runs from the deep (internal) inguinal ring — an opening in the transversalis fascia lying about 1.25 cm above the midpoint of the inguinal ligament — to the superficial (external) ring, a defect in the external oblique aponeurosis. Critically, recall that the inferior epigastric vessels run upwards from the external iliac vessels just medial to the deep ring; their position is the landmark that separates an indirect from a direct hernia. Recall also Hesselbach's triangle, bounded laterally by the inferior epigastric vessels, medially by the lateral border of rectus abdominis and inferiorly by the inguinal ligament — the weak area through which a direct hernia bulges. Finally recall the pubic tubercle, the bony landmark that separates a groin hernia into inguinal (above and medial to it) or femoral (below and lateral to it).
The Patient with a Groin Lump
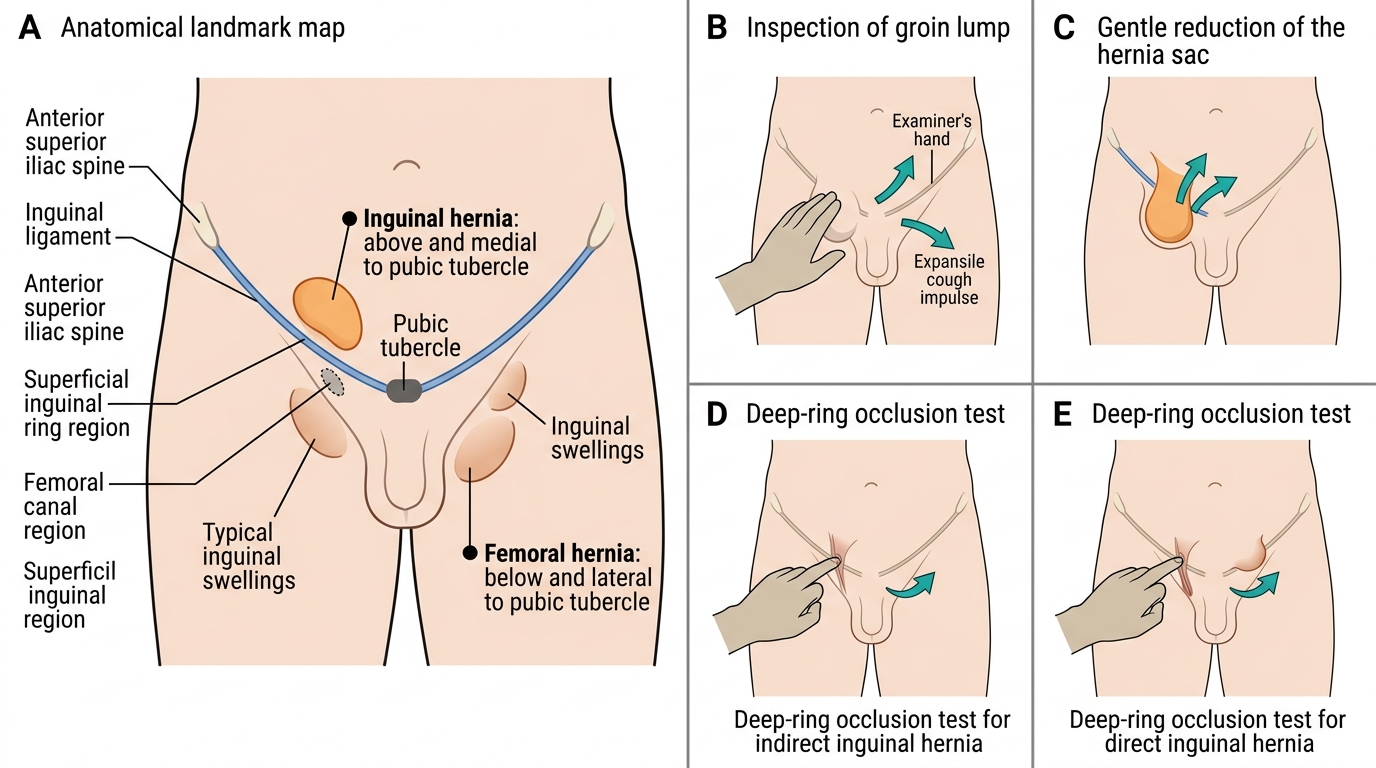
Most hernias present as a swelling that the patient notices, and the history alone takes you a long way. The classic uncomplicated hernia is a lump that appears or enlarges on standing, straining, coughing or lifting and reduces — disappears — on lying down, often with the patient demonstrating how they push it back themselves. A key positive sign on examination is an expansile cough impulse: when the patient coughs, the lump visibly and palpably expands, confirming its connection to the abdominal cavity. You must then actively search the history for the features that signal a hernia in trouble, because these change a planned operation into an emergency one. Ask whether the lump has become painful, whether it has stopped going back (irreducibility), and whether there are features of intestinal obstruction — colicky abdominal pain, distension, vomiting and absolute constipation — which together suggest that bowel within the sac is obstructed or strangulated. Note the site precisely: a lump in the groin may be inguinal or femoral, and a lump elsewhere on the abdominal wall (umbilical, epigastric, or at the scar of a previous operation) points to a different type. Ask about predisposing factors that raise intra-abdominal pressure or weaken the wall — chronic cough, constipation, straining at micturition (prostatism), heavy manual work, ascites, pregnancy and previous abdominal surgery. A clear history of a reducible lump with a cough impulse, with none of the warning features, describes the common, repairable hernia; any of the warning features demands urgent assessment.
Pathophysiology and Surgical Anatomy of Hernias
A hernia is the abnormal protrusion of a viscus, or part of a viscus, through a defect in the wall of the cavity that normally contains it. Every hernia has the same components: a sac (a pouch of peritoneum with a mouth, neck, body and fundus), its contents (most often small bowel or omentum), and the coverings derived from the layers of the wall it pushes through. Hernias arise where the wall is naturally weak or has been weakened — congenitally (a persistent processus vaginalis) or by acquired degeneration and raised intra-abdominal pressure. Groin hernias are the commonest and must be distinguished precisely. The indirect inguinal hernia passes through the deep inguinal ring, lateral to the inferior epigastric vessels, traversing the canal within the coverings of the cord; it is the commonest hernia overall, is usually congenital (a patent processus vaginalis), occurs in younger patients, and can descend into the scrotum. The direct inguinal hernia pushes forward through the weakened posterior wall of the canal in Hesselbach's triangle, medial to the inferior epigastric vessels; it is acquired, occurs in older patients with weak abdominal walls, and rarely enters the scrotum. The femoral hernia descends through the femoral canal, below and lateral to the pubic tubercle (below the inguinal ligament); it is commoner in women, has a narrow, rigid neck, and carries the highest risk of strangulation of the common hernias. Other important sites are umbilical/paraumbilical, epigastric and incisional hernias. The reason hernias matter clinically is the continuum of complications they follow: a reducible hernia returns to the abdomen; an irreducible (incarcerated) hernia cannot be pushed back but its contents are still viable; an obstructed hernia contains bowel whose lumen is blocked, causing intestinal obstruction; and a strangulated hernia is one in which the blood supply to its contents is cut off, leading to ischaemia, necrosis and, if untreated, perforation and peritonitis — a surgical emergency.
Provided image
Provided image
| Feature | Indirect inguinal | Direct inguinal | Femoral |
|---|---|---|---|
| Route | Through deep ring, along the canal | Through Hesselbach's triangle (posterior wall) | Through femoral canal |
| Relation to inferior epigastric vessels | Lateral | Medial | — (below inguinal ligament) |
| Relation to pubic tubercle | Above and medial | Above and medial | Below and lateral |
| Typical patient | Younger; congenital (patent processus) | Older; acquired wall weakness | Women; middle-aged/elderly |
| Descends to scrotum | Yes (can) | Rarely | No |
| Strangulation risk | Moderate | Low | High (narrow rigid neck) |
SELF-CHECK
An inguinal hernia that passes through the deep inguinal ring LATERAL to the inferior epigastric vessels and can descend into the scrotum is best classified as:
A. Direct inguinal hernia
B. Indirect inguinal hernia
C. Femoral hernia
D. Paraumbilical hernia
Reveal Answer
Answer: B. Indirect inguinal hernia
An indirect inguinal hernia enters through the deep ring LATERAL to the inferior epigastric vessels, travels down the inguinal canal within the cord coverings and can reach the scrotum; it is usually congenital. A direct hernia bulges through Hesselbach's triangle MEDIAL to the vessels and rarely reaches the scrotum. A femoral hernia lies below the inguinal ligament.
Examining the Hernia Patient and Investigations
The examination of a hernia is a disciplined routine performed with the patient first standing and then lying, with the groin and scrotum fully exposed. Inspect for the swelling, its site relative to the pubic tubercle, any change on coughing, and (in the scrotum) whether you can get above it. Ask the patient to cough and look for an expansile cough impulse. Palpate to define the lump, then try to reduce it gently — note whether it reduces and how. The single most useful anatomical test is to identify the pubic tubercle: an inguinal hernia emerges above and medial to it, whereas a femoral hernia lies below and lateral to it — this distinction is the cornerstone of groin examination. To separate an indirect from a direct inguinal hernia, reduce the hernia and perform the deep (internal) ring occlusion test: occlude the deep ring (1.25 cm above the mid-inguinal point) with a finger and ask the patient to cough — an indirect hernia is controlled and does not reappear, whereas a direct hernia, bulging forward through the posterior wall medial to the ring, still appears. Always examine both sides and complete the examination by examining the other hernial orifices, the external genitalia and the abdomen, and by checking for predisposing causes such as a chronic cough or an enlarged prostate. Investigations are usually unnecessary because the diagnosis is clinical, but when the diagnosis is uncertain (an occult hernia, an obese patient, or a possible femoral hernia in a groin lump) an ultrasound is the first imaging test, and CT is useful for complex, recurrent or incisional hernias and to plan repair; routine bloods are arranged before operation.
Examination of Groin Hernia
- Locate the pubic tubercle: inguinal = above and medial; femoral = below and lateral.
- Look for an expansile cough impulse; try to reduce the lump.
- Deep-ring occlusion test: controls an indirect hernia; a direct hernia still bulges.
- Examine both groins and complete with genitalia, abdomen and search for predisposing causes.