Page 8 of 20
SU28.15 | Appendicitis and Appendicular Complications — SDL Guide (Part 2)
Surgical Management and the Complications
The definitive treatment of acute appendicitis is appendicectomy, performed laparoscopically (now usual, with less wound infection and faster recovery) or open through a gridiron/Lanz incision, after resuscitation with intravenous fluids and prophylactic antibiotics. Early operation prevents perforation, and the diagnosis being primarily clinical, a reasonable rate of negative appendicectomy has traditionally been accepted to avoid missing the disease (though imaging has reduced it). Antibiotics alone can resolve some uncomplicated cases but with a significant recurrence rate, so surgery remains standard. Management of the complications is where precise knowledge pays off. Perforation with generalised peritonitis demands urgent resuscitation, antibiotics and operation (appendicectomy with peritoneal lavage). The crucial distinction is between the appendicular mass and the appendicular abscess. An appendicular mass (phlegmon) — a walled-off inflammatory mass with no drainable pus, found in a patient presenting a few days into the illness — is classically managed conservatively by the Ochsner–Sherren regimen: intravenous fluids, antibiotics, marking the limits of the mass and monitoring pulse, temperature and the mass size, allowing it to resolve, with an interval appendicectomy classically about six weeks later. Conservative management is abandoned — and the patient operated on — if the mass enlarges, the pain, temperature or pulse rise, or signs of peritonitis develop. An appendicular abscess (a collection of pus) is treated by drainage — radiologically guided percutaneous drainage or surgical drainage — with antibiotics, again often followed by interval appendicectomy. In all the special groups (pregnancy, elderly, children) the threshold to operate is lower because the consequences of delay are worse.
Provided image
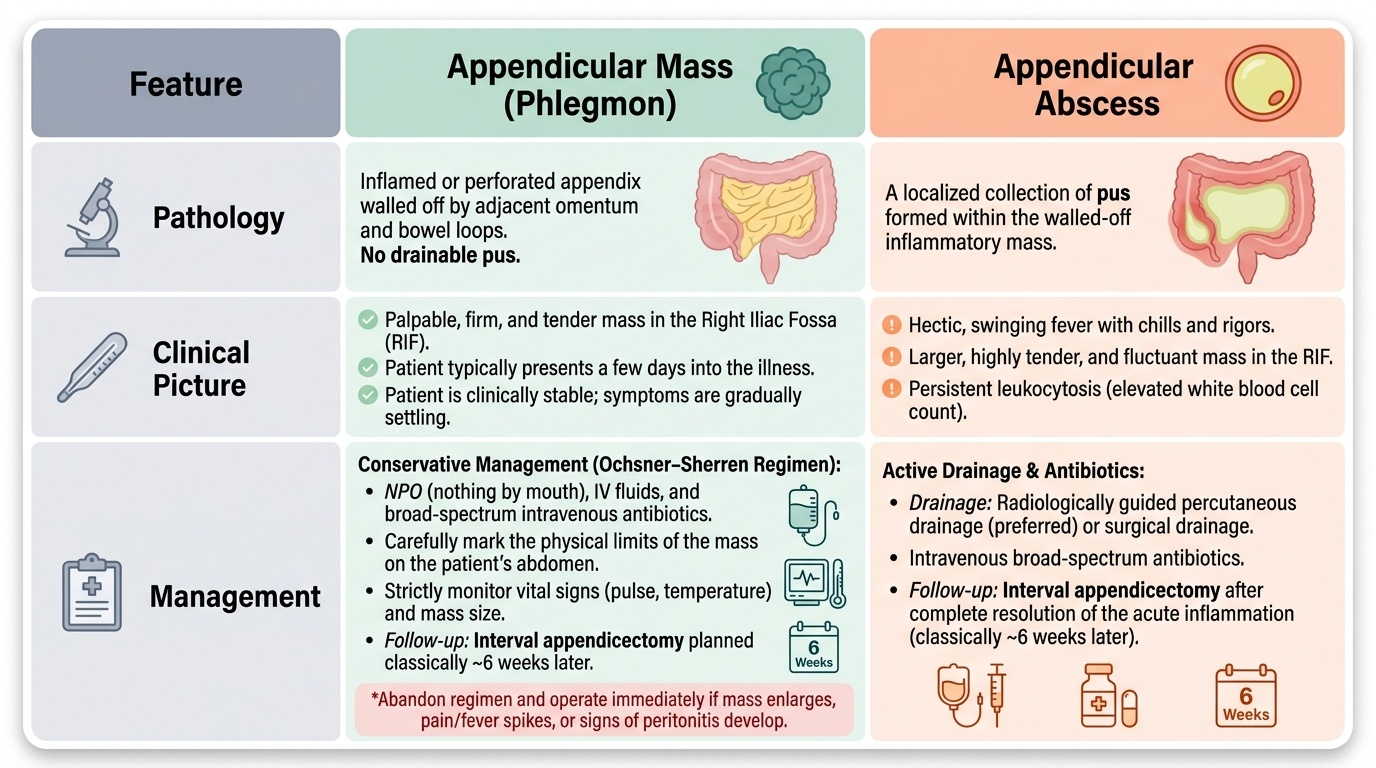
| Feature | Appendicular mass (phlegmon) | Appendicular abscess |
|---|---|---|
| Pathology | Inflamed/perforated appendix walled off by omentum and bowel; no drainable pus | A collection of pus within the walled-off area |
| Clinical picture | Palpable tender mass, settling, presents days into illness | Swinging fever, larger tender mass, toxic |
| Management | Conservative: Ochsner–Sherren regimen + interval appendicectomy | Drainage (percutaneous or surgical) + antibiotics (± interval appendicectomy) |
| Abandon conservative if | Mass enlarges, pain/temperature/pulse rise, or peritonitis develops | — (already needs drainage) |
CLINICAL PEARL
Anorexia and migratory pain are your best friends in diagnosing appendicitis — a genuinely hungry patient rarely has acute appendicitis. When a patient presents several days in with a tender right iliac fossa mass, stop and decide mass versus abscess before reaching for the knife: a settling phlegmon is managed conservatively by the Ochsner–Sherren regimen with interval appendicectomy, whereas a collection of pus needs drainage. And whatever the score or scan, never anchor on a 'normal' picture in a pregnant woman, an elderly patient or a young child — in these groups the classic story is muted and perforation is the rule of delay.
Check Your Understanding
Consolidate by reasoning back through the student in the hook and forward to the harder cases. His central pain migrating to the right iliac fossa with anorexia and nausea, tenderness and rebound at McBurney's point and a low-grade fever give a high Alvarado score and a confident clinical diagnosis of acute appendicitis — so after fluids and antibiotics he goes for appendicectomy before the end-artery supply lets the appendix perforate. Now stress-test the model: a woman of childbearing age needs a pregnancy test and an ultrasound to exclude ectopic and ovarian causes; a pregnant woman may have higher-than-expected pain because the uterus has displaced the appendix; an elderly patient may present late with few signs and a perforation. And a patient arriving four days into the illness with a tender mass requires the mass-versus-abscess decision. Self-test the three competency strands. First, can you give the classic and the atypical clinical features (pregnancy, elderly, children)? Second, can you outline the investigation — clinical scoring with Alvarado, bloods, selective ultrasound/CT — and the differential? Third, can you state the management of uncomplicated appendicitis and, critically, the difference between the Ochsner–Sherren management of an appendicular mass and the drainage of an abscess? The questions below check exactly these links.
SELF-CHECK
A patient presents 4 days after the onset of right iliac fossa pain with a tender, palpable mass but is otherwise settling, with a falling temperature and pulse. What is the appropriate initial management?
A. Immediate emergency appendicectomy
B. Conservative management by the Ochsner–Sherren regimen with monitoring and interval appendicectomy
C. Percutaneous drainage of the mass
D. Discharge with oral antibiotics and no follow-up
Reveal Answer
Answer: B. Conservative management by the Ochsner–Sherren regimen with monitoring and interval appendicectomy
A settling appendicular mass (phlegmon) with no drainable pus is managed conservatively by the Ochsner–Sherren regimen — IV fluids, antibiotics, marking and monitoring the mass and the pulse/temperature — with interval appendicectomy classically about 6 weeks later. Conservative management is abandoned only if the mass enlarges or the pain, temperature or pulse rise, or peritonitis develops. A frank abscess (pus) would instead need drainage.