Page 16 of 26
SU29.{6,8} | Renal Tumours and Bladder Cancer — SDL Guide
Learning Objectives
- Describe the clinical features, investigations and principles of management of renal tumours, including renal cell carcinoma and Wilms' tumour (SU29.6).
- Describe the clinical features, investigations and principles of management of bladder cancer, distinguishing non-muscle-invasive from muscle-invasive disease (SU29.8).
INSTRUCTIONS
Haematuria is the symptom that links the two commonest urological cancers a surgeon meets. Behind a solid mass in the flank usually lies a renal cell carcinoma; behind painless blood in the urine usually lies a bladder transitional cell carcinoma. Each is now a treatable disease when recognised and staged correctly, and each is defined by a small number of decisions: is the renal mass small enough to spare nephrons, has the bladder tumour invaded muscle, and what does the histology demand next. This module connects the presentation of renal and bladder tumours to a disciplined work-up and to the surgical and oncological choices that follow, so that visible blood in the urine triggers the right investigation rather than false reassurance.
References
- Bailey & Love's Short Practice of Surgery, The Kidneys and Ureters; The Urinary Bladder (textbook)
- SRB's Manual of Surgery, Genitourinary System — Renal Tumours and Bladder Tumours (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 58-year-old man has a CT scan of his abdomen after a road traffic collision. He has no urinary symptoms at all, yet the radiologist reports a 4 cm solid mass in the upper pole of his right kidney — an incidental finding that will change his life. In the next cubicle sits a 65-year-old retired dye-factory worker who has come because, twice in the last month, his urine has turned bright red and then cleared again, completely without pain. One patient has a tumour he never felt; the other has a warning sign he was almost tempted to ignore because it stopped hurting — or rather, never hurt at all. Both are sitting on a urological cancer, and the task of this module is to make sure that neither the silent renal mass nor the painless red urine is missed, mislabelled, or mismanaged.
WHY THIS MATTERS
Renal and bladder cancers are among the commonest solid tumours a general surgeon and urologist encounter, and both are curable when caught before they spread. The reason they matter so much for a final-year student is that each turns on a single, easily-missed clinical cue. For the kidney, the historic teaching of a 'classic triad' is a trap: by the time a renal cell carcinoma is felt as a mass, it is usually advanced, and the modern reality is that most are found incidentally on imaging — so a small, asymptomatic renal mass deserves urgent characterisation, not watchful neglect. For the bladder, the cue is even simpler and even more dangerous to dismiss: painless visible haematuria is bladder cancer until proven otherwise, and the commonest reason a curable tumour becomes incurable is that intermittent, painless bleeding was reassured away. Getting the work-up and the muscle-invasion question right is what separates a bladder preserved from a bladder removed, and a nephron spared from a kidney lost.
RECALL
Recall a few foundations before we build on them. From anatomy: the kidney has an outer cortex and inner medulla draining into the renal pelvis, and the nephron's proximal convoluted tubule is the epithelium from which renal cell carcinoma arises — while the renal pelvis and the entire urinary tract down to the bladder are lined by transitional epithelium (urothelium), which is why pelvis, ureter and bladder share the same family of urothelial cancers. The kidney drains via the renal vein into the inferior vena cava (IVC) on the right and (importantly for a clinical sign) the left renal vein receives the left gonadal (testicular) vein, so left renal vein obstruction can produce a left-sided varicocele. From physiology: the kidney secretes erythropoietin and renin, which explains some of the paraneoplastic effects of renal tumours. Hold on to one idea above all — that the whole urothelial lining behaves as a single field, so urothelial tumours are typically multifocal and recurrent, which shapes how we follow bladder cancer for life.
The Patient with Haematuria: Renal and Bladder Tumours
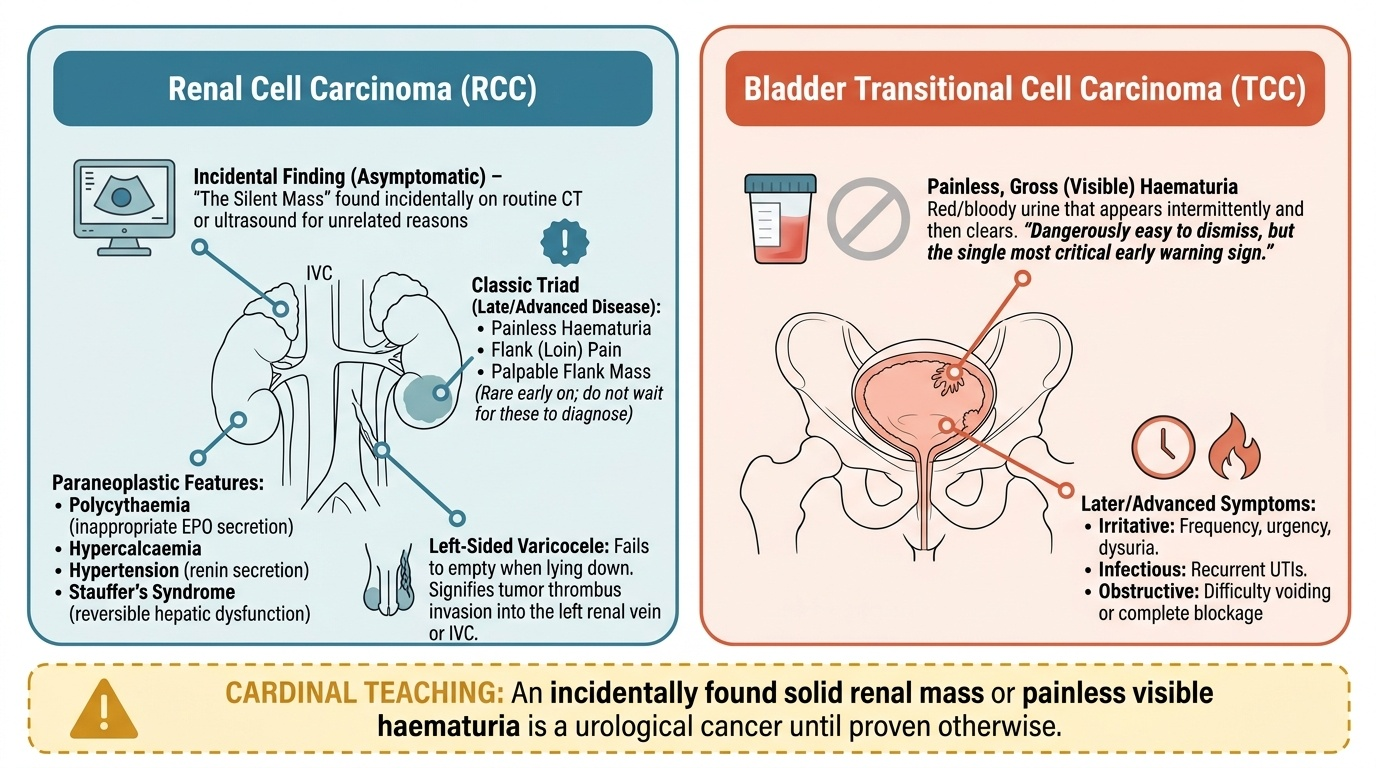
Renal and bladder tumours present in two characteristically different ways, and learning to recognise each presentation is the first step in not missing them. A renal cell carcinoma (RCC) today most often causes no symptoms at all and is discovered incidentally on an ultrasound or CT performed for some unrelated reason — the silent mass of the patient in the hook. The textbook classic triad of haematuria, flank (loin) pain and a palpable mass is in fact uncommon and, when present, signals late, advanced disease, so it must never be relied upon to make the diagnosis early. Beyond the triad, RCC is famous for its paraneoplastic syndromes: polycythaemia from inappropriate erythropoietin, hypercalcaemia, hypertension from renin secretion, and Stauffer's syndrome (a reversible non-metastatic hepatic dysfunction). A left-sided varicocele that does not empty on lying down is a classic clue to left renal vein or IVC involvement by tumour thrombus. In children the renal tumour to know is entirely different: Wilms' tumour (nephroblastoma) is the commonest renal tumour of childhood, typically presenting under the age of five as an abdominal mass found by a parent, sometimes with haematuria or hypertension. Bladder cancer, by contrast, announces itself far more simply. The hallmark presentation of bladder transitional cell carcinoma is painless, gross (visible) haematuria — blood that appears in the urine, often intermittently, and then clears, with no pain to accompany it. Because the bleeding is painless and comes and goes, it is dangerously easy to dismiss, yet it is the single most important early sign. Later or more advanced disease may add irritative symptoms (frequency, urgency, dysuria), recurrent infections, or symptoms of obstruction. The cardinal teaching that anchors this whole topic is therefore simple: an incidentally found solid renal mass and painless visible haematuria are each a urological cancer until proven otherwise.
Provided image
- Renal cell carcinoma: most are now incidental imaging findings; the classic triad (haematuria + flank pain + palpable mass) is uncommon and indicates late disease.
- RCC red flags: paraneoplastic features (polycythaemia, hypercalcaemia, hypertension, Stauffer's syndrome); left-sided non-emptying varicocele (renal vein/IVC involvement).
- Wilms' tumour: commonest renal tumour of children (under ~5 yr) — abdominal mass +/- haematuria/hypertension.
- Bladder cancer: painless gross (visible) haematuria is the hallmark; later disease may add frequency, urgency, dysuria or obstruction.
Pathology and Surgical Basis of Renal and Bladder Tumours
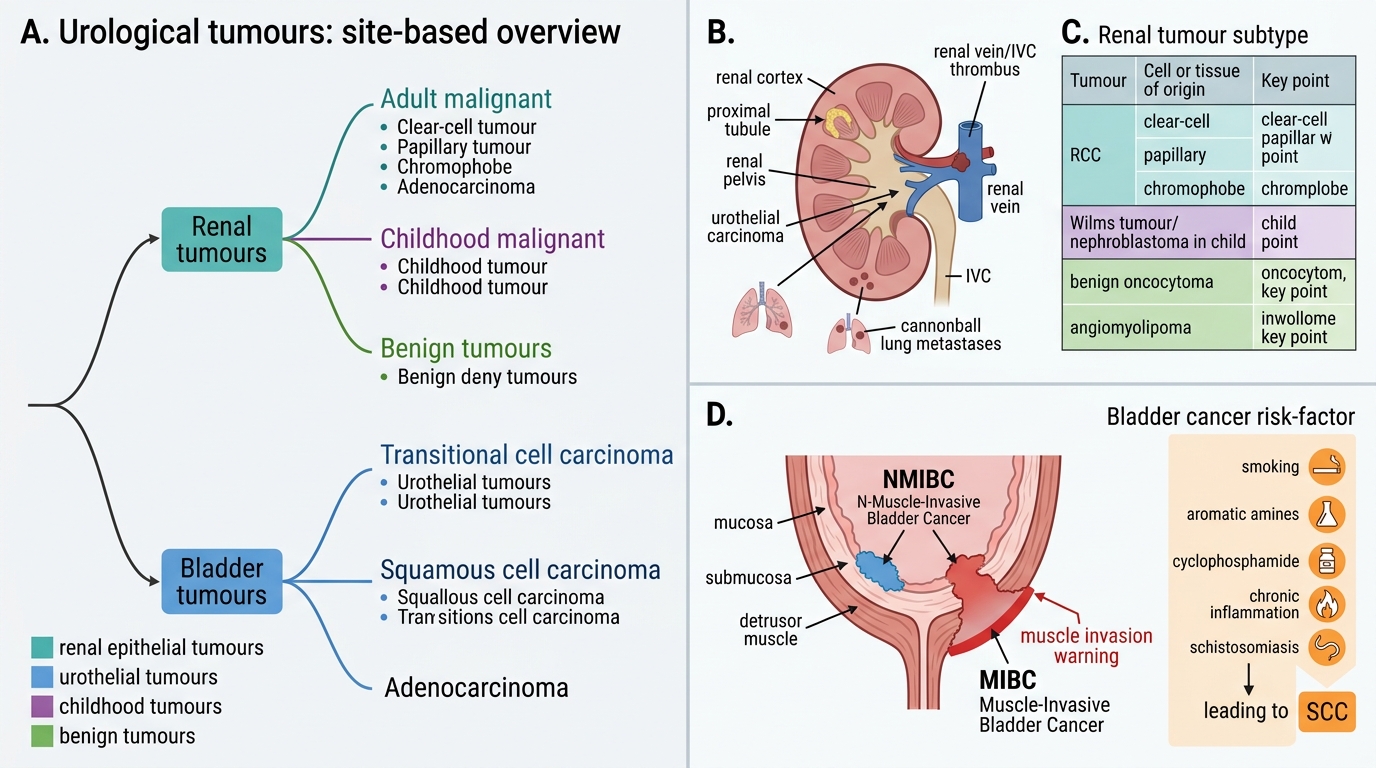
The surgery of these tumours follows directly from their pathology, so the classification must be clear. Among renal tumours, the dominant adult malignancy is renal cell carcinoma (RCC), which arises from the epithelium of the proximal convoluted tubule; its clear-cell subtype is by far the most common, with papillary and chromophobe subtypes accounting for most of the remainder. RCC characteristically grows into the renal vein and may extend as a tumour thrombus up the inferior vena cava, and it spreads haematogenously to the lung (producing rounded 'cannonball' metastases) and to bone; it is also notably relatively radio- and chemo-resistant, a fact that dictates a surgical and targeted-therapy approach rather than conventional chemoradiation. Distinct from RCC, the renal pelvis is lined by urothelium and can give rise to transitional cell (urothelial) carcinoma, the same cancer family as the bladder. The childhood tumour, Wilms' tumour (nephroblastoma), is an embryonal tumour of a quite different biology and prognosis. Benign renal tumours worth naming are oncocytoma and angiomyolipoma. Among bladder tumours, the commonest type in both the West and India is transitional cell (urothelial) carcinoma (TCC), whose major risk factors are smoking (the single most important), occupational exposure to aromatic amines (aniline dyes, rubber industry), the drug cyclophosphamide, and chronic inflammation. A crucial exception to remember is that chronic infection with schistosomiasis (Schistosoma haematobium) causes squamous cell carcinoma (SCC) of the bladder in endemic regions such as Egypt and parts of Africa and the Middle East; adenocarcinoma is rarer. The single most important pathological distinction for management is the depth of invasion, which divides bladder cancer into non-muscle-invasive bladder cancer (NMIBC) — confined to mucosa/submucosa — and muscle-invasive bladder cancer (MIBC), which has invaded the detrusor muscle; this distinction, made on the resected specimen, decides whether the bladder can be preserved or must be removed.
⚑ AI image — pending faculty review (auto-QA score 5/10; best of 3 attempts)
Classification of Renal and Bladder Tumours
- Renal tumours (adult, malignant): RCC (clear-cell commonest; from proximal tubule; renal vein/IVC thrombus; cannonball lung mets; radio-/chemo-resistant); urothelial TCC of the renal pelvis.
- Renal tumour (child): Wilms' tumour (nephroblastoma) — commonest renal tumour of childhood.
- Benign renal: oncocytoma, angiomyolipoma.
- Bladder cancer: TCC commonest (smoking, aromatic amines, cyclophosphamide, chronic inflammation); schistosomiasis -> SCC; adenocarcinoma rare.
- Key surgical divide: NMIBC (mucosa/submucosa) versus MIBC (detrusor muscle invaded) determines bladder preservation versus cystectomy.
SELF-CHECK
A 60-year-old smoker presents with painless visible haematuria. Which single tumour type is most likely, and what is the key pathological feature that will determine whether his bladder can be preserved?
A. Squamous cell carcinoma; whether schistosome ova are present
B. Transitional cell carcinoma; whether the tumour has invaded the detrusor muscle
C. Adenocarcinoma; whether the urachus is involved
D. Renal cell carcinoma; whether the renal vein contains tumour thrombus
Reveal Answer
Answer: B. Transitional cell carcinoma; whether the tumour has invaded the detrusor muscle
Painless gross haematuria in a smoker is bladder transitional cell carcinoma (TCC) until proven otherwise — smoking is the major risk factor. The decisive pathological feature is depth of invasion: non-muscle-invasive disease (NMIBC) can be managed with bladder-preserving TURBT plus intravesical therapy, whereas muscle-invasive disease (MIBC) usually needs radical cystectomy. Schistosomiasis causes squamous cell carcinoma (a different type), and renal vein thrombus is a feature of renal cell carcinoma, not bladder cancer.
Examination and Investigation
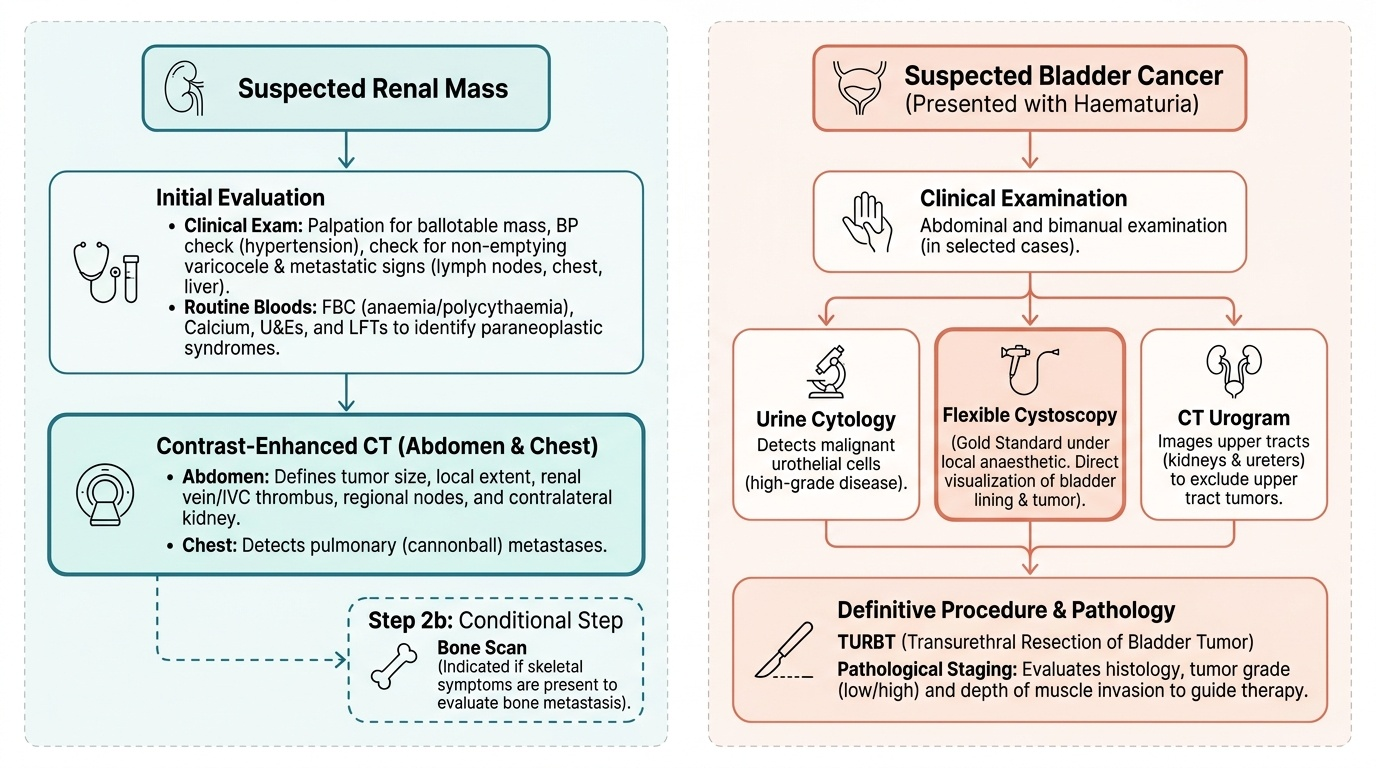
Clinical examination of these patients is often unremarkable, which is precisely why investigation is the heart of the work-up — but it should still be performed systematically. For a suspected renal tumour, palpate both loins for a ballotable mass, percuss and auscultate, examine for a non-emptying varicocele (especially left-sided), look for signs of metastatic disease (hepatomegaly, bony tenderness, cervical nodes, chest signs) and check blood pressure (renin-driven hypertension). The investigation of a renal mass is essentially radiological: a contrast-enhanced CT of the abdomen is the key investigation for characterising and staging the tumour, defining its size and local extent, demonstrating renal vein or IVC tumour thrombus, and assessing the regional nodes and the contralateral kidney; a CT of the chest completes staging by looking for pulmonary (cannonball) metastases, and a bone scan is added if symptoms suggest skeletal spread. Routine bloods (full blood count for polycythaemia or anaemia, calcium, renal and liver function) may reveal the paraneoplastic picture. For a patient with haematuria suspected of bladder cancer, the examination includes abdominal and (in selected cases) bimanual examination, but the diagnosis is made cystoscopically. Flexible cystoscopy is the gold-standard investigation: it directly visualises the bladder lining and any tumour, and can be performed under local anaesthetic in the clinic. It is supported by urine cytology (which can detect malignant urothelial cells, especially in high-grade disease) and by CT urogram, which images the upper tracts (kidneys and ureters) to exclude synchronous upper-tract urothelial tumours given the field-change nature of the disease. The definitive staging step is transurethral resection of bladder tumour (TURBT): the visible tumour is resected endoscopically, and the specimen — which must include the underlying muscle — provides the histological diagnosis, the tumour grade, and most importantly the depth of invasion that separates NMIBC from MIBC. In short, the renal mass is characterised by cross-sectional imaging, while the bladder tumour is diagnosed and staged by cystoscopy and TURBT.
Provided image
- Renal mass: contrast CT abdomen is the key staging test (size, local extent, renal vein/IVC thrombus, nodes) + CT chest for lung mets (+/- bone scan); bloods for paraneoplastic features.
- Bladder cancer: flexible cystoscopy = gold standard; urine cytology adjunct; CT urogram assesses the upper tracts (field change).
- TURBT: endoscopic resection giving histology, grade, and depth of invasion — the step that classifies NMIBC vs MIBC.