Page 5 of 26
SU29.3 | Urinary Tract Infections — SDL Guide (Part 2)
Principles of Surgical Management
Management of urinary tract infection follows directly from where the patient sits on the spectrum, and the surgeon's contribution is to recognise and treat the causes and complications that drugs cannot reach. Uncomplicated lower UTI in a healthy non-pregnant woman is treated with a short, usually empirical course of an appropriate antibiotic, later refined by culture and sensitivity. Acute pyelonephritis needs more aggressive antibiotic therapy, often initially intravenous, together with fluids and analgesia, and the septic patient is resuscitated along sepsis-management lines — early broad-spectrum antibiotics, fluids, and source control. The single most important surgical principle in this whole topic is this: an obstructed, infected urinary system must be decompressed urgently, and antibiotics alone will not save it. A pyonephrosis — pus trapped behind an obstruction — is relieved without delay by percutaneous nephrostomy (a tube placed into the collecting system through the flank) or by a retrograde ureteric stent, restoring drainage so that antibiotics can finally work and the kidney can be saved; the obstructing cause (commonly a stone) is dealt with definitively only after the infection has been controlled. Pus elsewhere obeys the same ancient surgical law — a perinephric or renal abscess is drained, percutaneously or operatively. Emphysematous pyelonephritis, the gas-forming necrotising infection of the diabetic kidney, demands intensive resuscitation, glycaemic control and broad-spectrum antibiotics, with drainage for many and nephrectomy for the worst cases that do not respond. Fournier's gangrene is the most time-critical of all: it requires immediate, aggressive surgical debridement of all necrotic tissue, repeated as needed, alongside broad-spectrum antibiotics and full resuscitation; delay is measured in lives lost. Two further principles complete the picture. First, asymptomatic bacteriuria — a positive culture in a patient with no symptoms — is generally NOT treated, because treatment confers no benefit and breeds resistance; the important exceptions are pregnancy (where it risks pyelonephritis and preterm labour) and before urological instrumentation or surgery (to prevent septic complications), in which cases it should be treated. Second, catheter-associated infection is managed by removing or changing the catheter alongside antibiotics where there is true infection rather than mere colonisation. Above everything, the rule for the complicated, recurrent, or male UTI is to find and treat the underlying urological abnormality — the stone, the stricture, the obstructing prostate or tumour — because an infection that has a surgical cause will keep returning until that cause is corrected.
Provided image
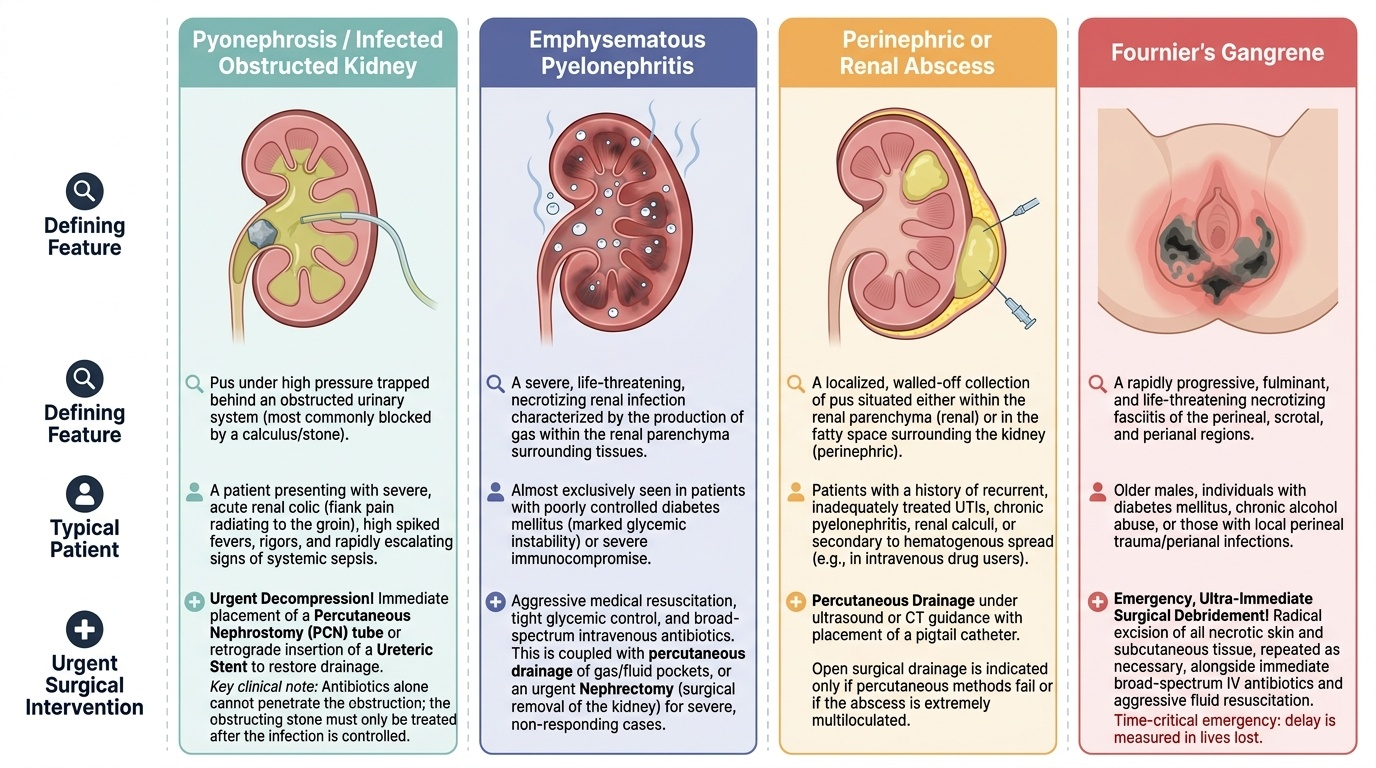
- Antibiotics guided by culture; resuscitate the septic patient (early antibiotics, fluids, source control).
- Decompress urgently an obstructed infected system — percutaneous nephrostomy or ureteric stent for pyonephrosis; treat the obstructing cause only after infection is controlled.
- Drain perinephric/renal abscesses; emphysematous pyelonephritis → resuscitation + drainage ± nephrectomy; Fournier's gangrene → immediate aggressive debridement.
- Asymptomatic bacteriuria: treat ONLY in pregnancy or before urological instrumentation; otherwise do not treat.
- Always investigate and treat the underlying abnormality in complicated, recurrent or male UTI.
CLINICAL PEARL
When a febrile patient with a urinary tract infection is not improving on appropriate antibiotics, assume there is undrained pus or an obstructed infected system until imaging proves otherwise — and image urgently. An infected obstructed kidney (pyonephrosis) is a closed-space infection: the antibiotic cannot reach the urine behind the blockage, the patient stays septic, and the kidney is destroyed while you wait. The correct reflex is not a stronger antibiotic but a drain — percutaneous nephrostomy or a ureteric stent — restoring flow first and treating the cause (usually a stone) afterwards. 'Antibiotics first, then drainage' is exactly the wrong order for an obstructed infected system.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The young woman with isolated dysuria, frequency and suprapubic ache, systemically well and with a structurally normal tract, has an uncomplicated lower UTI: a dipstick, a midstream culture and a short course of an appropriate antibiotic, with no imaging required, is correct and sufficient. The diabetic man with loin pain, rigors, falling blood pressure, drowsiness and an ultrasound showing a kidney full of debris behind an obstructing stone has a pyonephrosis with urosepsis — a urological emergency in which resuscitation and urgent decompression by percutaneous nephrostomy or ureteric stent, not a change of antibiotic, will save his life and his kidney. Use these contrasting cases to self-test the competency this module covers. First, can you classify a UTI along the three axes the surgeon uses — uncomplicated versus complicated, lower versus upper, and the special states including asymptomatic bacteriuria and the surgical emergencies — and say who counts as complicated? Second, can you state what defines significant bacteriuria on culture, and when asymptomatic bacteriuria should and should not be treated? Third, can you name the four surgical/urological emergencies of the infected urinary tract and the urgent intervention each requires, and can you recite the cardinal rule that an obstructed infected system must be decompressed before antibiotics can work? The questions that follow check exactly these links.
SELF-CHECK
A 60-year-old diabetic man has high fever, severe left loin pain and early hypotension. Ultrasound shows a dilated, debris-filled left collecting system behind an obstructing ureteric stone. After resuscitation and intravenous antibiotics, what is the most important immediate step?
A. Escalate to a broader-spectrum intravenous antibiotic and observe
B. Urgent decompression of the kidney by percutaneous nephrostomy or ureteric stent
C. Immediate open removal of the ureteric stone
D. Immediate nephrectomy of the affected kidney
Reveal Answer
Answer: B. Urgent decompression of the kidney by percutaneous nephrostomy or ureteric stent
This is a pyonephrosis — an infected, obstructed kidney — which is a urological emergency. Antibiotics cannot reach pus trapped behind an obstruction, so the kidney must be decompressed urgently by percutaneous nephrostomy or a retrograde ureteric stent. The obstructing stone is dealt with definitively only after the infection has been controlled; escalating antibiotics alone or rushing to definitive stone surgery or nephrectomy first is wrong.