Page 7 of 17
SU30.3-5 | Epididymo-Orchitis, Varicocele and Hydrocele — SDL Guide
Learning Objectives
- Describe the applied anatomy, clinical features, investigations and principles of management of epididymo-orchitis (SU30.3).
- Describe the applied anatomy, clinical features, investigations and principles of management of varicocele (SU30.4).
- Describe the applied anatomy, clinical features, investigations and principles of management of hydrocele (SU30.5), and in every acute painful scrotum exclude testicular torsion first.
INSTRUCTIONS
Scrotal swellings and scrotal pain are everyday surgical and urological presentations, and three benign conditions account for most of them — an inflamed, infected epididymis (epididymo-orchitis), a dilated vein plexus that feels like a bag of worms (varicocele), and a fluid collection around the testis you can transilluminate (hydrocele). The clinician's job is twofold: characterise the swelling with a few disciplined bedside tests, and in any acutely painful scrotum first exclude the one diagnosis that cannot wait — testicular torsion. This module ties the scrotal anatomy and venous drainage to those bedside signs, the focused investigations, and the principles of treatment for each condition.
References
- Bailey & Love's Short Practice of Surgery, The Testis and Scrotum / Urology (textbook)
- SRB's Manual of Surgery, The Scrotum and Testis (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three men present to the same on-call shift with scrotal complaints. A 28-year-old has a tender, swelling left hemiscrotum that has come on over two days, with a fever and a burning when he passes urine; lifting the testis seems to ease his pain. A 19-year-old, by contrast, comes in with the sudden, severe pain of half an hour ago in a high-riding, exquisitely tender testis, vomiting, and no relief from anything — and your alarm bells ring. A third, a 32-year-old, has noticed a soft, painless, slowly enlarging swelling that lights up like a lantern when you shine a torch through it. Three scrotums, three very different stories, and your first and overriding question with every painful scrotum is the same: have I excluded the testicular torsion that needs the operating theatre within hours?
WHY THIS MATTERS
These conditions matter both because they are common and because one impostor among them is a surgical emergency. Epididymo-orchitis is the usual cause of an acutely inflamed scrotum and responds to the right antibiotic — but it shares its presentation with testicular torsion, and the price of mistaking torsion for infection is a lost testis, so the safe rule is to exclude torsion in every acute painful scrotum. Varicocele is important because, beyond the dragging discomfort and 'bag of worms' it produces, it is a recognised and treatable contributor to male subfertility, and a new right-sided one in an older man can be the first clue to a renal tumour. Hydrocele is usually benign, but the discipline of working out whether you can 'get above' the swelling, whether it transilluminates, and whether a tumour lurks beneath a secondary hydrocele is exactly the kind of bedside reasoning a final-year student is examined on. Mastering the three swellings — and the torsion you must never miss — equips you for one of the commonest scenarios in surgical practice.
RECALL
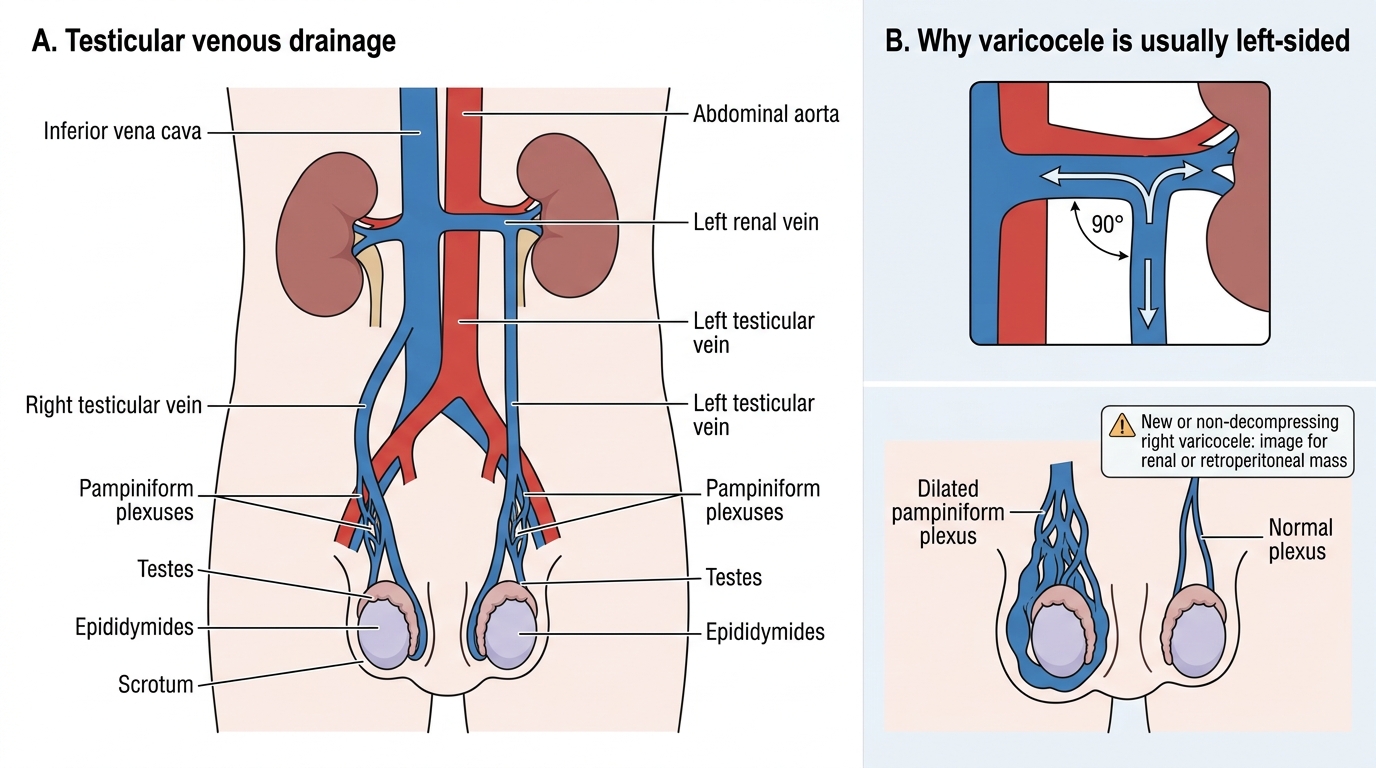
Recall the relevant anatomy before applying it. The testis and epididymis are invested by the tunica vaginalis, a closed serous sac derived from the processus vaginalis, whose two layers normally hold only a film of fluid — an imbalance of secretion and absorption here produces a hydrocele. The testis is drained by a network of veins, the pampiniform plexus, which ascends in the spermatic cord and condenses into the testicular (gonadal) vein; crucially, the right testicular vein drains directly into the inferior vena cava, while the left drains into the left renal vein, joining it at a right angle — anatomy that explains why varicoceles are overwhelmingly left-sided. The cremasteric reflex (afferent and efferent limbs in the genitofemoral nerve) normally elevates the testis when the inner thigh is stroked; its absence is an important sign of torsion. Hold on to one safety idea: in the acute painful scrotum, anatomy and signs help you separate inflammation from the mechanical catastrophe of torsion, but uncertainty should send the patient to theatre, not home.
The Patient with a Scrotal Swelling or Pain
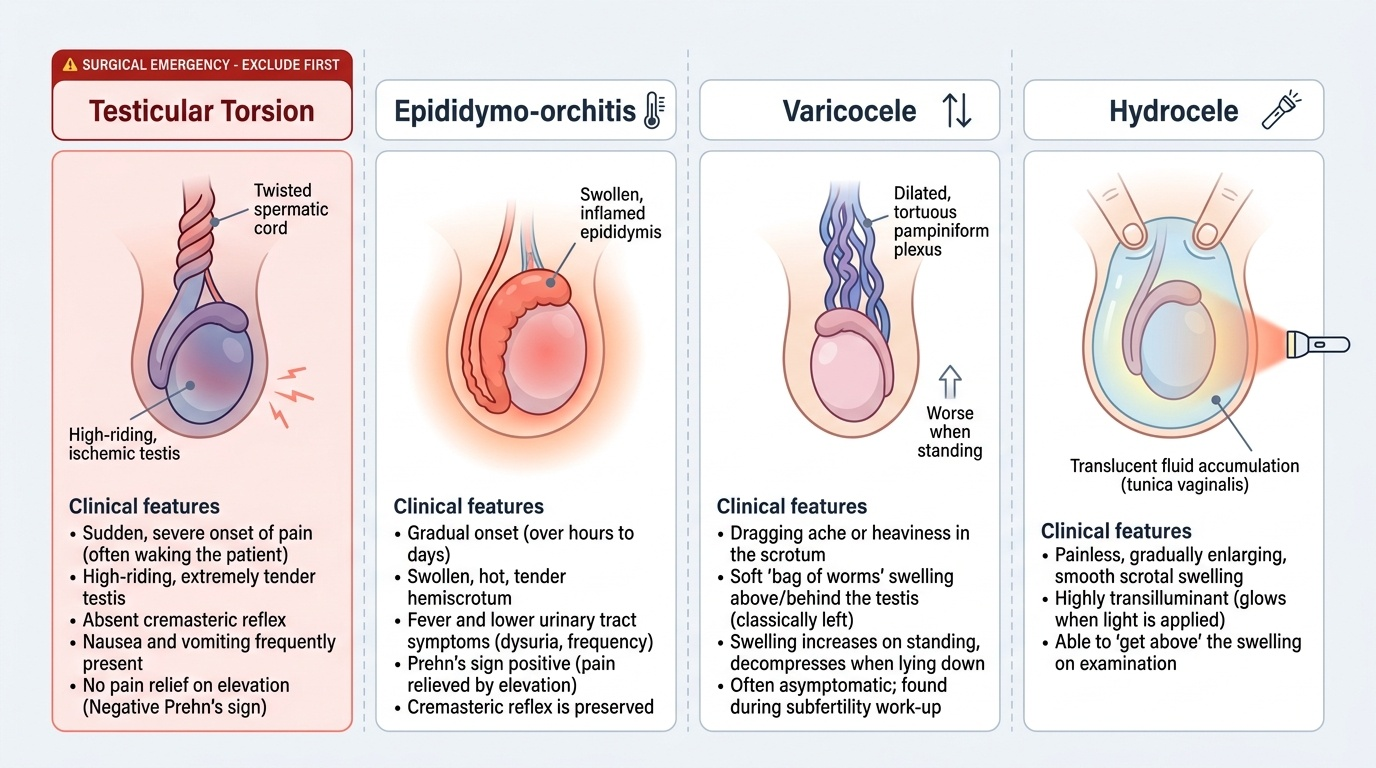
The three conditions, and the emergency they hide among, separate largely on the history and the tempo of onset. Epididymo-orchitis typically presents with gradual onset over hours to a day or two of a swollen, hot, tender hemiscrotum, often with fever and lower urinary tract symptoms (dysuria, frequency) or a urethral discharge, reflecting an ascending infection; classically, elevating the testis relieves the pain (Prehn's sign positive) and the cremasteric reflex is preserved. Varicocele presents quite differently as a dragging ache or heaviness in the scrotum, worse on standing and towards the end of the day, or it is found during a subfertility work-up; the patient or examiner notices a soft, 'bag of worms' swelling above and behind the testis, almost always on the left, which becomes more prominent on standing and decompresses on lying down. Hydrocele presents as a painless, gradually enlarging scrotal swelling; it is transilluminant, and you can get above it (the examining fingers meet above the swelling), which distinguishes it from an inguinoscrotal hernia. Standing apart from all three is testicular torsion — the can't-miss diagnosis — which presents with sudden, severe pain (often waking the patient or following exertion), a tender, high-riding testis, an absent cremasteric reflex, frequently nausea/vomiting, and no relief on elevation; it is commonest in adolescents and is a surgical emergency in which delay loses the testis. The first discipline, therefore, is always to ask: is this the torsion I must exclude?
Provided image
- Epididymo-orchitis: gradual onset, fever/dysuria, Prehn's sign positive, cremasteric reflex preserved.
- Varicocele: dragging ache or subfertility, left-sided 'bag of worms', worse standing.
- Hydrocele: painless, transilluminant, can get above it.
- Testicular torsion (exclude first!): sudden severe pain, high-riding tender testis, absent cremasteric reflex — surgical emergency.
Applied Anatomy and Pathological Basis
Each swelling has a tidy anatomical and pathological explanation. Epididymo-orchitis is almost always an ascending infection from the urethra or bladder along the vas to the epididymis (and then the testis); the likely organism depends on age and sexual history — in young, sexually active men it is usually a sexually transmitted organism (Chlamydia trachomatis or Neisseria gonorrhoeae), whereas in older men, boys, or those with urinary tract obstruction or instrumentation it is usually a urinary coliform (Escherichia coli). Varicocele is a dilatation and tortuosity of the pampiniform plexus caused by incompetent or absent venous valves and the column of blood it must support. Its strong left-sided predominance follows directly from the recall anatomy: the left testicular vein drains into the left renal vein at a right angle (a longer, higher-resistance course, and the point where the renal vein can be compressed between the aorta and superior mesenteric artery), whereas the right drains obliquely straight into the IVC. This is also why a new, isolated, non-decompressing right-sided varicocele — or any varicocele that does not empty on lying down — should prompt imaging to exclude a renal or retroperitoneal mass obstructing the vein. Hydrocele is an abnormal collection of serous fluid within the tunica vaginalis, arising from an imbalance between fluid secretion and absorption; a primary (idiopathic) hydrocele has no underlying cause, while a secondary hydrocele forms in response to an underlying problem such as infection, trauma, or — importantly — a testicular tumour, which is why the testis must always be assessed. For completeness, testicular torsion results from twisting of the spermatic cord (often on a 'bell-clapper' congenital anomaly), which strangles the venous then arterial supply — the mechanism behind its emergency status.
Testicular Venous Drainage and Left-Sided Varicocele
- Epididymo-orchitis: ascending infection — STI organisms (Chlamydia/gonococcus) in young men, coliforms (E. coli) in older men/UTI.
- Varicocele: dilated pampiniform plexus from valvular incompetence; left-sided because the left testicular vein enters the left renal vein at a right angle; a non-decompressing or new right varicocele → image for a renal/retroperitoneal mass.
- Hydrocele: fluid within the tunica vaginalis; primary (idiopathic) vs secondary (infection, trauma, tumour) — always assess the underlying testis.
SELF-CHECK
A 16-year-old presents with sudden severe left scrotal pain of one hour, a high-riding tender testis, an absent cremasteric reflex and vomiting. What is the correct immediate action?
A. Start antibiotics for epididymo-orchitis and review in 48 hours
B. Arrange an outpatient Doppler ultrasound and analgesia at home
C. Treat as testicular torsion and proceed to urgent surgical exploration without delaying for imaging if the diagnosis is clinically suspected
D. Reassure and elevate the testis to relieve the pain
Reveal Answer
Answer: C. Treat as testicular torsion and proceed to urgent surgical exploration without delaying for imaging if the diagnosis is clinically suspected
This is testicular torsion — sudden severe pain, a high-riding tender testis and an absent cremasteric reflex in a teenager. Testicular salvage depends on time (best within about 6 hours), so when torsion is clinically suspected the patient goes to urgent surgical exploration; imaging must not delay theatre. Treating it as epididymo-orchitis or sending the patient home risks losing the testis.
Examination and Investigation
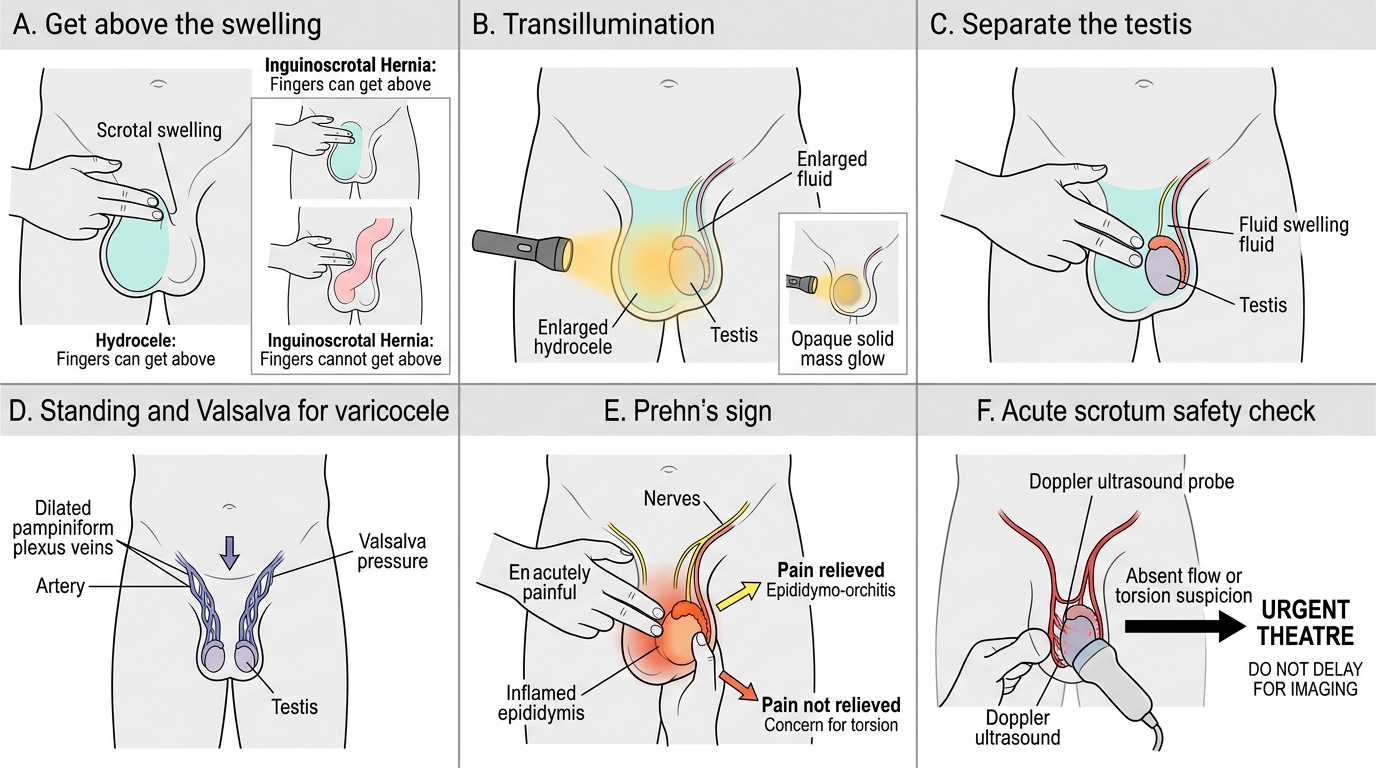
A short set of disciplined bedside tests sorts most scrotal swellings, and the investigations are then targeted. Begin by deciding whether you can get above the swelling: if your fingers meet above it at the neck of the scrotum, the swelling is confined to the scrotum (hydrocele, epididymal or testicular lesions); if you cannot, suspect an inguinoscrotal hernia. Transilluminate in a darkened room — a hydrocele lights up brightly (a fluid-filled swelling), whereas a solid tumour or a thick-walled chronic hydrocele does not. Try to palpate the testis separately from the swelling — possible with a varicocele or a small hydrocele, but a tense hydrocele may obscure the testis (mandating ultrasound to exclude an underlying tumour). For suspected varicocele, examine the standing patient and ask him to perform a Valsalva manoeuvre — the 'bag of worms' becomes more obvious and should decompress on lying down. For the acute painful scrotum, the key signs are Prehn's sign (relief on elevation suggests epididymo-orchitis; no relief suggests torsion), the cremasteric reflex (preserved in epididymo-orchitis, absent in torsion), and the position of the testis (high-riding in torsion). Investigations follow the suspicion: urinalysis and urine culture, with an STI screen/urethral swab in young men, for epididymo-orchitis; a scrotal Doppler ultrasound, which both characterises swellings and — critically — assesses testicular blood flow to help confirm or exclude torsion (but it must never delay theatre when torsion is clinically obvious); and a semen analysis when a varicocele is being assessed for subfertility. Remember that secondary hydrocele demands you look beneath it: scan the testis for a tumour.
Clinical Examination Signs in Scrotal Swelling
- Bedside tests: get-above-it (hydrocele vs hernia), transillumination (hydrocele lights up), separate the testis, standing/Valsalva for varicocele, Prehn's sign and cremasteric reflex for the acute scrotum.
- Investigations: urinalysis/culture + STI screen (epididymo-orchitis); scrotal Doppler ultrasound (characterise swelling, assess flow — but do not delay theatre for torsion); semen analysis (varicocele subfertility).
- Always assess the underlying testis in a hydrocele (scan to exclude a tumour in a secondary hydrocele).