Page 1 of 17
SU30.1 | Phimosis, Paraphimosis and Carcinoma Penis — SDL Guide
Learning Objectives
- Describe the clinical features, investigations and principles of management of phimosis, paraphimosis and carcinoma penis (SU30.1).
- Recognise paraphimosis as a urological emergency and outline its immediate reduction.
- Identify the risk factors for carcinoma penis and outline its staging and management principles, including inguinal node assessment.
INSTRUCTIONS
Three of the commonest reasons a male patient is referred for a penile problem sit on a single anatomical theme — the foreskin and the glans it covers. A foreskin that will not retract is phimosis; a retracted foreskin that becomes trapped behind the glans and swells is paraphimosis, a true emergency; and an ulcer or lump on the glans or prepuce, often arising in a chronically diseased, unretractable foreskin, is carcinoma of the penis. Learning the three together makes the thread explicit: chronic foreskin disease and poor hygiene link the trivial to the malignant, and a quick, confident bedside diagnosis decides whether you reassure, operate tonight, or refer for cancer work-up.
References
- Bailey & Love's Short Practice of Surgery, The Penis and Scrotum / Urology (textbook)
- SRB's Manual of Surgery, The Penis (textbook)
- Sabiston Textbook of Surgery, Urologic Surgery (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three men sit in your clinic in one afternoon. The first is the worried father of a four-year-old whose foreskin 'still won't pull back' — the boy is otherwise well and passes urine in a normal stream. The second is a 24-year-old who retracted his foreskin in the shower hours ago and now has an exquisitely painful, swollen glans with a tight band of skin choking it from behind; he cannot pull the skin forward again. The third is a 62-year-old who has finally come because a 'sore' on the end of his penis has not healed for three months and now bleeds and smells, and he has never been circumcised. The same small piece of anatomy — the foreskin — is at the heart of all three, but the urgency could not be more different: one needs reassurance, one needs your hands within minutes, and one needs a cancer pathway today.
WHY THIS MATTERS
These conditions matter because the cost of getting them wrong is high and avoidable. Paraphimosis is genuinely time-critical: a foreskin trapped behind the glans acts like a tourniquet, and progressive oedema can tip into ischaemia and even necrosis of the glans if reduction is delayed — recognising it and reducing it is a skill every clinician on call must have. Carcinoma penis, though uncommon where neonatal circumcision is routine, is devastating when missed, and its strongest modifiable risk factors — chronic phimosis, smegma retention and poor hygiene — are exactly what you will see in the phimosis clinic, so the benign and the malignant share a waiting room. For a final-year student these are classic examination topics: you are expected to define each precisely, separate physiological from pathological phimosis, and state why a penile ulcer demands biopsy and an inguinal node examination rather than a course of antibiotics.
RECALL
Recall the relevant anatomy before building on it. The penis has three erectile columns — the paired corpora cavernosa dorsally and the single corpus spongiosum ventrally, which surrounds the urethra and expands distally to form the glans. The glans is normally covered by the prepuce (foreskin), a double fold of skin tethered ventrally by the frenulum; the prepuce is separated from the glans by the preputial sac, where shed cells and secretions form smegma. Wrapping the erectile bodies is the deep fascia of the penis, Buck's fascia, an important barrier that limits the local spread of penile cancer. Hold on to one more fact for later: the skin of the penis and the glans drain their lymph first to the inguinal lymph nodes, which is why examining the groins is part of examining any penile lesion.
The Patient with a Foreskin or Penile Problem
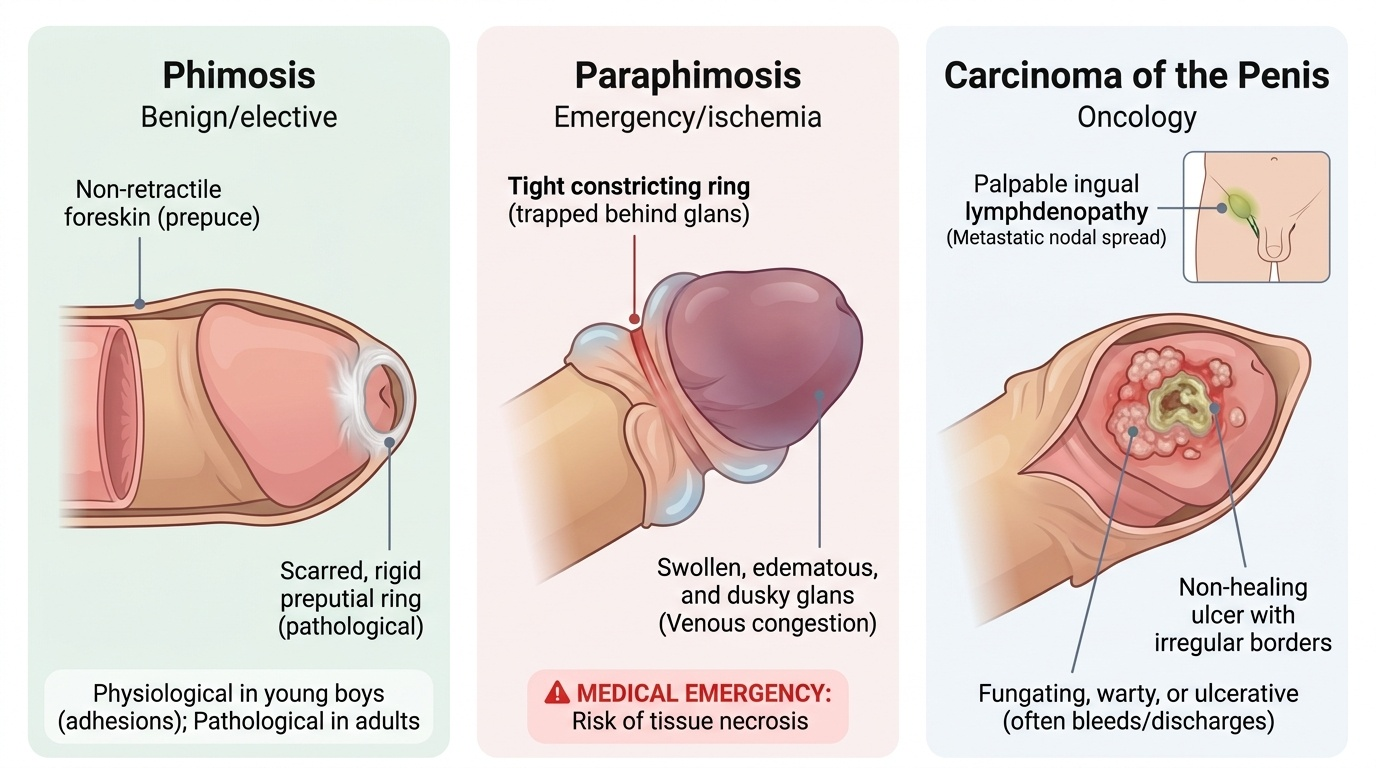
The three conditions announce themselves with very different stories, and the history almost makes the diagnosis. Phimosis is the inability to retract the prepuce over the glans. In young boys this is usually physiological — the prepuce is naturally non-retractile in infancy because of normal adhesions and a narrow opening, and it gradually frees up over the first years of life — so the presentation is a parent's concern rather than a sick child, provided the urinary stream is normal and there is no ballooning or recurrent infection. Pathological phimosis in older boys and adults presents instead with a scarred, white, rigid preputial ring that will not retract, often with soreness, splitting on erection, recurrent balanitis, spraying of urine or, in severe cases, obstruction. Paraphimosis is the opposite mechanical problem and a far more dramatic presentation: the foreskin has been retracted behind the glans — during washing, catheterisation or intercourse — and a tight constricting ring now prevents it being drawn forward again, so the patient comes in distressed with a painful, progressively swollen, dusky glans. Carcinoma penis presents most often as a non-healing ulcer or a warty/fungating lesion on the glans or inner prepuce, sometimes hidden under a phimotic foreskin until it bleeds, discharges or smells; there may be a palpable lump in the groin from nodal spread. The cardinal triage question is simple — is this the emergency (paraphimosis), the elective benign problem (phimosis), or the cancer (a non-healing penile lesion)?
Provided image
- Phimosis: non-retractile foreskin; physiological in young boys, pathological (scarred ring, BXO) in adults.
- Paraphimosis: retracted foreskin trapped behind the glans, painful swelling — an emergency.
- Carcinoma penis: non-healing ulcer/fungating lesion on glans or prepuce, often with a groin lump.
Anatomy and the Pathological Basis of Penile Disease
Each condition makes sense once the anatomy and pathology are clear. Phimosis is fundamentally a problem of the preputial opening being too tight to pass over the glans. In infancy this is the normal, physiological state and needs no treatment beyond gentle hygiene and reassurance. Pathological adult phimosis is usually cicatricial — the result of scarring — and a very common cause is balanitis xerotica obliterans (BXO), the genital form of lichen sclerosus, which produces a characteristic white, atrophic, fibrosed preputial ring (and can also stricture the meatus). Recurrent balanitis and forcible early retraction can also scar the prepuce. Paraphimosis is a vicious mechanical cycle: once a tight foreskin is retracted behind the corona, the constricting band obstructs venous and lymphatic return from the glans and distal prepuce, so they become oedematous; the swelling tightens the band further, and if unrelieved the rising pressure can eventually compromise the arterial supply and threaten the glans with ischaemia — which is why it is an emergency. Carcinoma penis is a squamous cell carcinoma in over 95% of cases. Its aetiology is dominated by chronic irritation and inflammation of the glans and inner prepuce: retained smegma, poor hygiene and long-standing phimosis are classic risk factors, alongside infection with high-risk human papillomavirus (HPV 16 and 18), smoking, and premalignant conditions such as BXO and erythroplasia of Queyrat. The single most striking epidemiological fact is protective: neonatal circumcision virtually abolishes the disease, which is consequently rare in populations circumcised at birth. The tumour begins on the glans or prepuce, and Buck's fascia initially limits its deep spread before it invades the corpora.
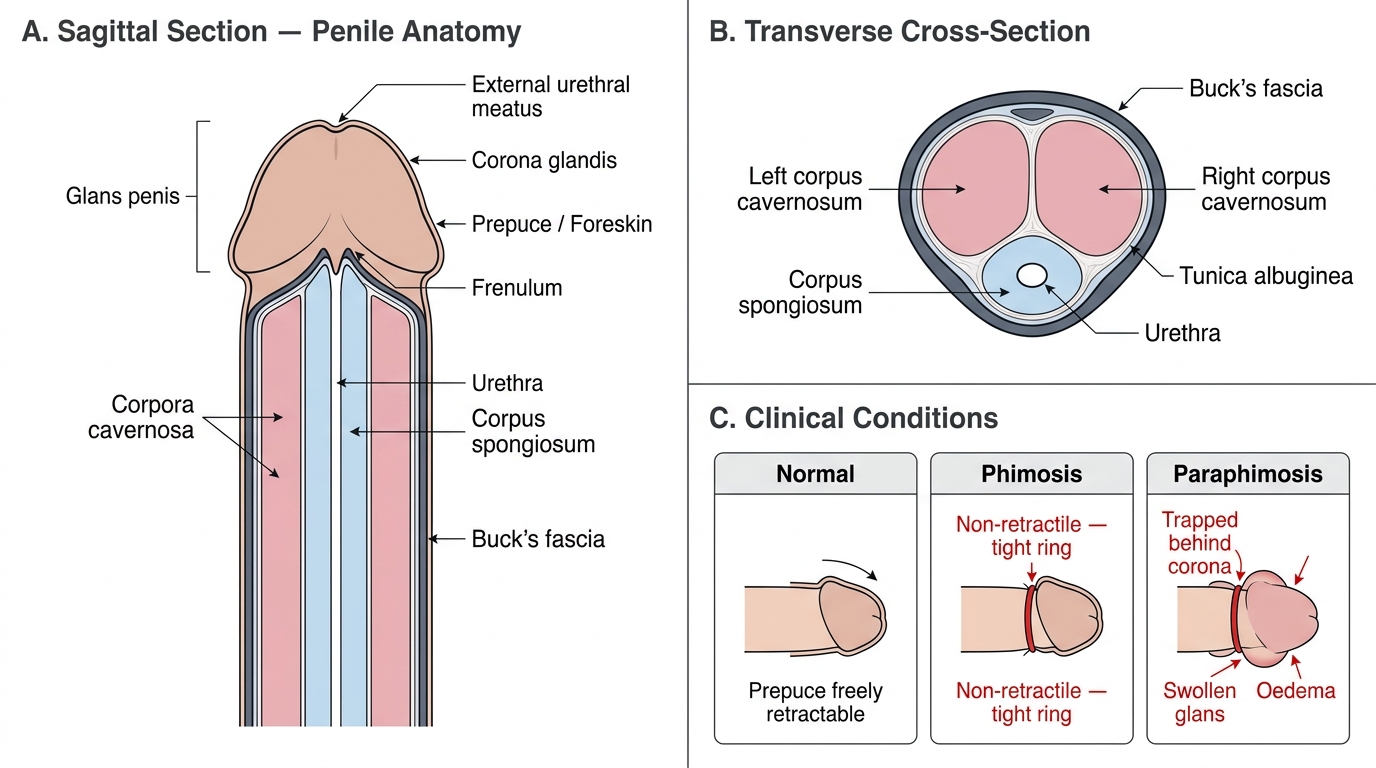
Penile Anatomy: Sagittal Section, Cross-Section, and Clinical Foreskin Conditions
- Phimosis: physiological (infants) vs pathological/cicatricial (BXO/lichen sclerosus, recurrent balanitis).
- Paraphimosis: constricting ring → venous/lymphatic obstruction → oedema → potential ischaemia.
- Carcinoma penis: SCC; risks = smegma, poor hygiene, phimosis, HPV 16/18; neonatal circumcision protective.
SELF-CHECK
A 24-year-old presents with a painful, swollen glans and a tight band of retracted foreskin trapped behind it that he cannot pull forward. What is the most appropriate immediate concern?
A. It is a self-limiting condition that will settle with reassurance
B. It is a urological emergency because progressive oedema can lead to glans ischaemia
C. It is most likely carcinoma penis and needs urgent biopsy
D. It is physiological phimosis and needs no treatment
Reveal Answer
Answer: B. It is a urological emergency because progressive oedema can lead to glans ischaemia
This is paraphimosis — a retracted foreskin trapped behind the glans. The constricting ring obstructs venous and lymphatic return, causing progressive oedema that can compromise the arterial supply and threaten the glans with ischaemia. It is a urological emergency requiring prompt reduction, not reassurance; it is distinct from phimosis (non-retractile foreskin) and from carcinoma.
Examination and Investigation
Examination is directed by which of the three you suspect, but a disciplined penile examination is the same each time and always includes the groins. Inspect the shaft, prepuce and — by gentle retraction where possible — the glans and coronal sulcus, looking for a scarred preputial ring, the white atrophic changes of BXO, balanitis, or an ulcer or warty growth; note any bleeding, discharge or fixation. Palpate any lesion for size, induration and depth, and assess whether it is confined to the skin/glans or appears to invade the corpora. In paraphimosis the diagnosis is visual and immediate — a swollen, often dusky glans with the foreskin bunched behind it — and you should not delay treatment to investigate. For phimosis little investigation is needed beyond confirming the diagnosis and screening for diabetes (a common contributor to recurrent balanitis). For a suspected carcinoma, the indispensable step is biopsy of the lesion to confirm squamous cell carcinoma and assess its grade and depth, because management hinges on histology — never simply treat a non-healing penile ulcer as an infection. Crucially, examine both groins for inguinal lymphadenopathy, since the penis drains first to the inguinal nodes and nodal status is the most important prognostic factor; palpable nodes may be reactive (from infection of the ulcer) or metastatic, so they are reassessed after a short course of antibiotics and confirmed by imaging or biopsy. Local staging uses MRI (or ultrasound) of the penis to gauge corporal invasion, and cross-sectional imaging (CT/PET) assesses pelvic nodes and distant spread.
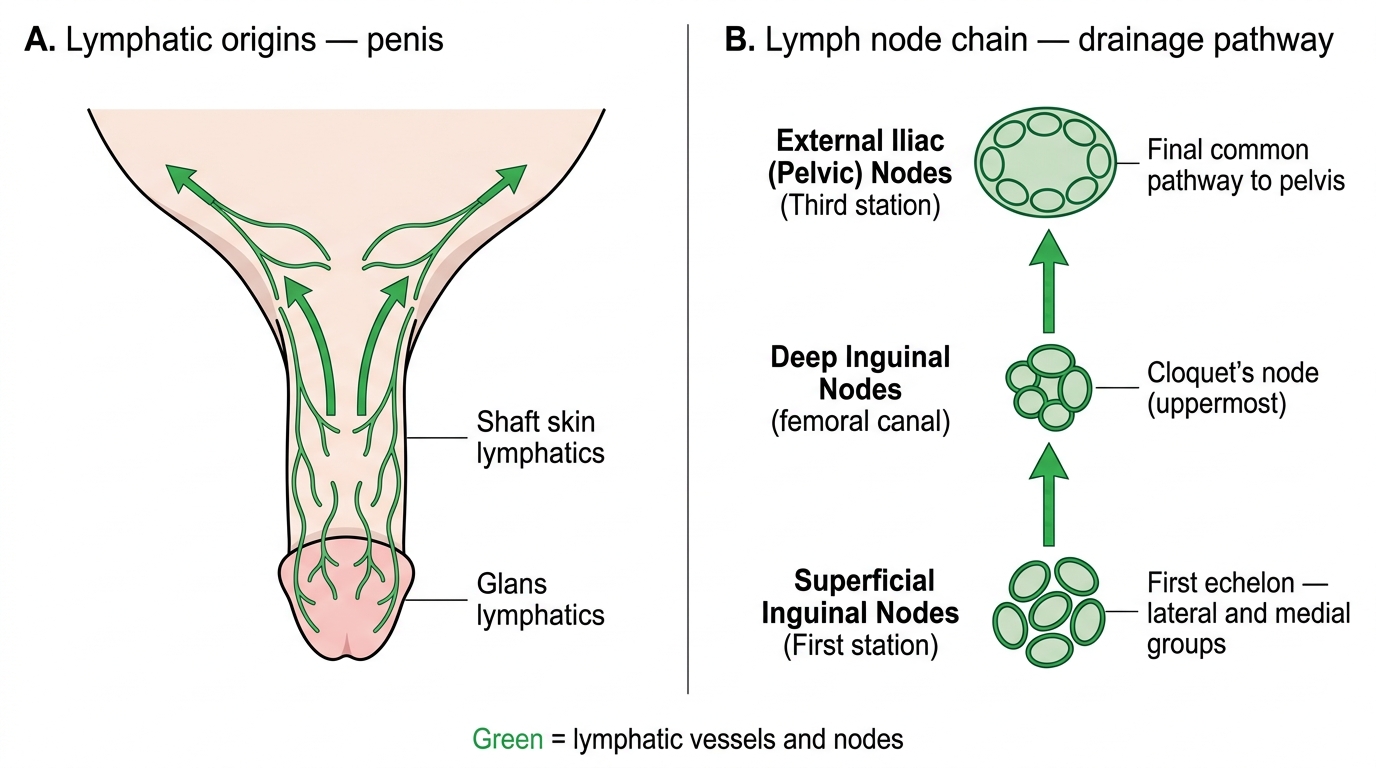
Penile Lymphatic Drainage Pathway
- Always biopsy a non-healing penile ulcer/lesion — do not treat blindly as infection.
- Always examine both groins — inguinal nodal status is the key prognostic factor.
- Staging: MRI for local (corporal) extent; CT/PET for pelvic nodes and distant disease.