Page 11 of 17
SU30.6 | Tumours of Testis — SDL Guide (Part 2)
Principles of Management
Management begins with surgery that is both diagnostic and therapeutic and then adds stage- and type-directed treatment. The first step for a solid intratesticular tumour is a radical inguinal orchidectomy — the spermatic cord is clamped and ligated high at the deep inguinal ring before the testis is mobilised, and the whole testis is delivered through the groin, never the scrotum, so that tumour is not spilled and the lymphatic drainage is not disturbed. Before any treatment, the man is offered sperm banking (cryopreservation), because both the disease and its treatment can impair fertility, and a testicular prosthesis can be offered for cosmesis. Histology of the specimen, the post-operative marker trend and the staging CT then guide adjuvant therapy. Seminoma is highly radiosensitive and chemosensitive, so stage-appropriate options include surveillance, radiotherapy to the para-aortic nodes, or chemotherapy. NSGCT is managed with chemotherapy and, in selected cases, retroperitoneal lymph node dissection (RPLND) for residual nodal masses; teratomatous residue in particular is resistant to chemotherapy and may need surgical removal. The workhorse chemotherapy for germ-cell tumours is the platinum-based BEP regimen (bleomycin, etoposide, cisplatin), and it is the reason testicular GCTs — even when metastatic — are among the most curable solid cancers, with cure rates that justify aggressive, protocol-driven treatment. Follow-up relies on serial tumour markers and imaging to detect relapse early, exploiting the same markers that characterised the tumour at the outset.
Provided image
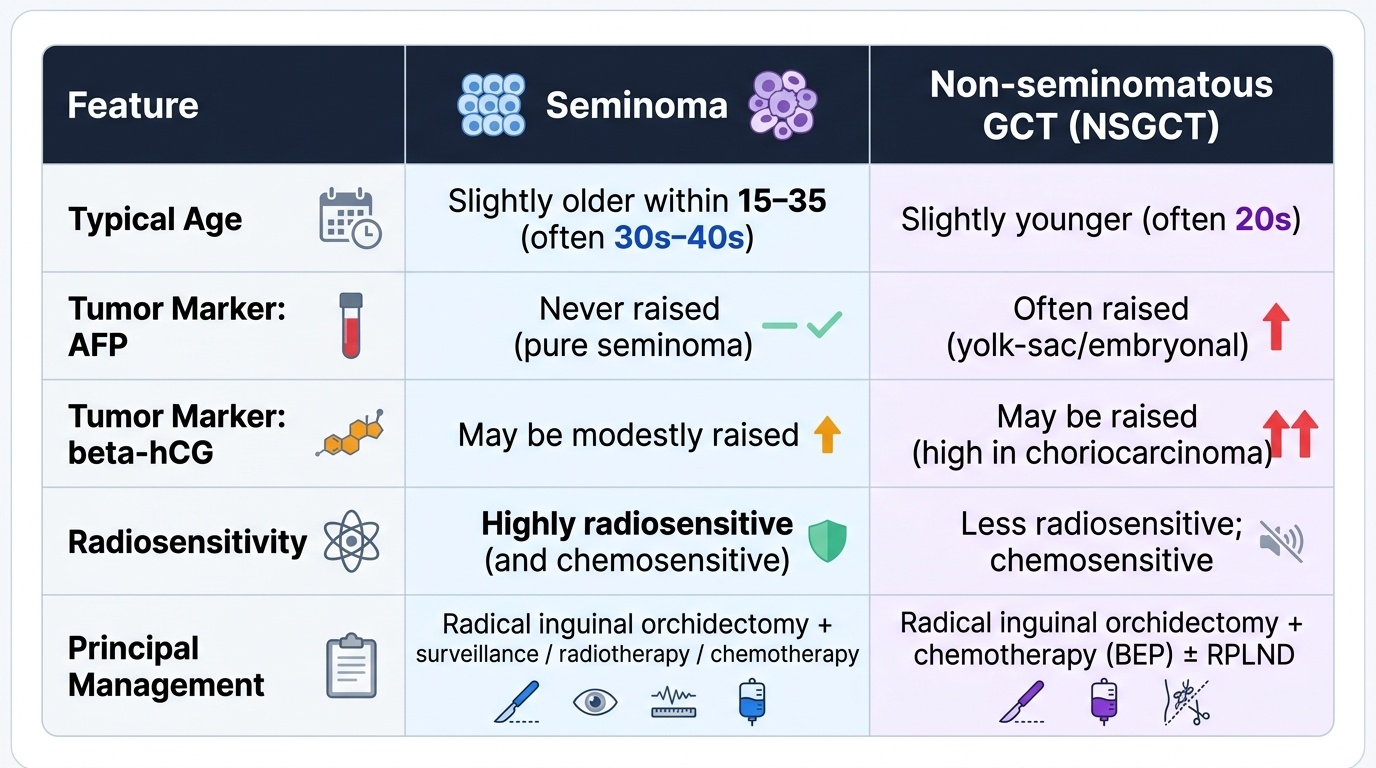
| Feature | Seminoma | Non-seminomatous GCT (NSGCT) |
|---|---|---|
| Typical age | Slightly older within 15–35 (often 30s–40s) | Slightly younger (often 20s) |
| AFP | Never raised (pure seminoma) | Often raised (yolk-sac/embryonal) |
| beta-hCG | May be modestly raised | May be raised (high in choriocarcinoma) |
| Radiosensitivity | Highly radiosensitive (and chemosensitive) | Less radiosensitive; chemosensitive |
| Principal management | Radical inguinal orchidectomy + surveillance/radiotherapy/chemotherapy | Radical inguinal orchidectomy + chemotherapy (BEP) ± RPLND |
CLINICAL PEARL
Two rules save testicular-cancer patients. First, NEVER perform a trans-scrotal biopsy or approach a testicular tumour through the scrotum — the diagnosis is made by removing the whole testis via a radical INGUINAL orchidectomy with high cord ligation, because breaching the scrotum seeds tumour and diverts lymphatic drainage from the para-aortic to the inguinal nodes, worsening the outlook. Second, interpret the markers precisely: a raised AFP means the tumour is NOT a pure seminoma (so it is treated as NSGCT), beta-hCG may be raised in seminoma and is high in choriocarcinoma, and LDH reflects tumour bulk. And before any treatment, offer sperm banking.
Check Your Understanding
Return to the 27-year-old footballer and trace the whole pathway. His painless, firm, craggy lump that you cannot get above and that does not transilluminate is a solid intratesticular mass — and in a man of 15–35 that is a germ-cell cancer until proven otherwise, so reasoning runs from 'solid testicular lump in a young man' to 'urgent cancer pathway, not reassurance'. You would examine his abdomen and nodes, request a scrotal ultrasound, send AFP, beta-hCG and LDH before any surgery, and stage with a CT chest/abdomen/pelvis — and you would explicitly not biopsy through the scrotum. You would offer sperm banking, perform a radical inguinal orchidectomy with high cord ligation, and let the histology, the falling markers and the staging CT direct adjuvant radiotherapy or chemotherapy (BEP) — reassuring him, truthfully, that even advanced germ-cell tumours are usually curable. Now self-test the competency directly. Can you classify testicular tumours (germ-cell seminoma vs NSGCT subtypes; sex-cord stromal; lymphoma in the elderly) and name the main risk factor (cryptorchidism)? Can you interpret AFP, beta-hCG and LDH — especially that AFP is never raised by a pure seminoma? Can you list the investigations in order and justify why the testis drains to the para-aortic nodes and why a trans-scrotal approach is forbidden? And can you state the principles of management — radical inguinal orchidectomy, sperm banking, and type-directed chemotherapy/radiotherapy? The questions that follow check these links.
SELF-CHECK
Why is the surgical treatment of a testicular tumour a radical INGUINAL orchidectomy rather than a scrotal approach or biopsy?
A. Because the inguinal approach is technically easier
B. Because the testis drains to the para-aortic nodes, and breaching the scrotum can seed tumour and divert drainage to the inguinal nodes, worsening prognosis
C. Because a scrotal incision heals more slowly
D. Because the inguinal approach allows the contralateral testis to be removed simultaneously
Reveal Answer
Answer: B. Because the testis drains to the para-aortic nodes, and breaching the scrotum can seed tumour and divert drainage to the inguinal nodes, worsening prognosis
The testis drains via its lymphatics to the para-aortic (retroperitoneal) nodes, while the scrotal skin drains to the inguinal nodes. A trans-scrotal biopsy or incision can seed tumour into the scrotum and divert lymphatic spread to the inguinal nodes, altering staging and worsening prognosis. The standard is therefore a radical inguinal orchidectomy with high ligation of the cord, removing the whole testis through the groin.