Page 7 of 14
SU6.1-2 | Surgical Infection and Antibiotic Management — SDL Guide
Learning Objectives
- Define surgical infection and describe its aetiology and pathogenesis in terms of the pathogen, the host and the local environment (SU6.1).
- Recognise the common types of surgical infection — surgical-site infection, cellulitis, abscess, necrotizing fasciitis, gas gangrene — and the organisms responsible (SU6.1).
- State the principle of source control and its primacy over antibiotics in established surgical infection (SU6.2).
- Enumerate prophylactic and therapeutic antibiotics and plan their appropriate use, including the timing rules of surgical prophylaxis (SU6.2).
INSTRUCTIONS
Despite sterile theatres and modern antibiotics, infection remains one of the commonest and most consequential complications of surgery — and some surgical infections, untreated for even a few hours, are lethal. This module explains why surgical infections happen (the balance between the pathogen, the host and the wound environment), the forms they take, and the two pillars of their management: source control and the rational use of antibiotics, prophylactic and therapeutic. It completes the cluster's progression from how wounds heal, through how wounds are classified and managed, to what happens — and what to do — when a wound becomes infected.
References
- Bailey & Love's Short Practice of Surgery, Surgical Infection chapter (textbook)
- SRB's Manual of Surgery, Surgical Infections and Antibiotics (textbook)
- Sabiston Textbook of Surgery, Surgical Infections and the Use of Antibiotics (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old diabetic man returns four days after an emergency operation. His wound, which looked fine on discharge, is now red, swollen, hot and exquisitely tender, and a bead of pus appears when the surgeon presses the edge. He has a fever and a rising pulse. On the ward two beds away lies a younger man whose leg, only twelve hours after a minor injury, has become tensely swollen, dusky and agonisingly painful out of all proportion to its appearance, with crackling under the skin and a patient who looks gravely unwell. One of these infections will resolve with simple drainage and a course of antibiotics; the other will kill within hours unless taken to theatre immediately. Telling them apart, understanding why each arose, and knowing that the knife — not the antibiotic — is the primary treatment of both, is the substance of this module.
WHY THIS MATTERS
Surgical infection sits at the centre of surgical safety. It prolongs admissions, breaks down wounds, threatens prostheses and grafts, and in its fulminant forms — necrotizing fasciitis, gas gangrene — kills quickly. Understanding its aetiology lets you predict and prevent it; recognising its types lets you act fast when minutes matter; and grasping the principle that source control comes before antibiotics prevents the lethal error of treating an undrained abscess or a spreading necrotizing infection with antibiotics alone. Rational antibiotic use — the right drug, the right indication, the right timing for prophylaxis, and the discipline not to over-prescribe — protects both the individual patient and the wider problem of resistance. SU6.1 and SU6.2 together turn infection from an unpredictable misfortune into something the surgeon anticipates, recognises and treats by sound principle.
RECALL
Before going further, recall what the previous SDLs in this cluster established. First, infection is one of the local factors that impair wound healing — it prolongs the inflammatory phase, consumes oxygen and nutrients, and separates healing edges. Second, the CDC surgical wound classification grades wounds by contamination (clean, clean-contaminated, contaminated, dirty) precisely because contamination predicts the risk of surgical-site infection. Third, source control concepts you have already met — debridement of dead tissue, removal of foreign material and drainage — are the mechanical removal of the soil in which infection grows. Also recall from basic science the acute inflammatory response and the host's immune defences. Keep these in mind: surgical infection is what happens when bacterial contamination overwhelms host defences in a favourable local environment, and its management is the application of these familiar principles under pressure.
Why Surgical Infection Matters
A surgical infection is, broadly, an infection that either requires surgical treatment (such as an abscess that must be drained) or that arises as a consequence of a surgical procedure (such as a surgical-site infection after an operation). It remains one of the most common and most important complications in surgical practice, accounting for a large share of postoperative morbidity, prolonged hospital stay and cost, and — in its severe forms — mortality. For the surgeon this matters on two levels. First, infection is largely predictable and preventable: it follows from identifiable risk factors and is reduced by sound asepsis, good surgical technique, control of the patient's comorbidities and the judicious use of prophylaxis. Second, when infection does occur, its outcome depends heavily on early recognition and prompt correct treatment, because the spectrum runs from a trivial stitch abscess to a fulminant necrotizing infection that is lethal within hours. The single most important conceptual point, which runs through everything that follows, is that the cornerstone of treating an established surgical infection is source control — draining pus, excising dead tissue, removing infected foreign material — with antibiotics as an important but secondary adjunct. Understanding this prevents the commonest and most dangerous mistake in managing surgical infection: relying on antibiotics while the source festers.
Aetiology and Pathogenesis: Pathogen, Host and Environment
Whether a wound becomes infected is determined by a balance, classically expressed as the interplay of three factors: the pathogen, the host and the local environment. On one side sits the bacterial challenge — the number (dose) of organisms delivered to the wound and their virulence (their capacity to invade and damage tissue, and to evade defences). On the other side sits host resistance — systemic immunity, which is impaired by diabetes, malnutrition, immunosuppression, steroids, extremes of age and obesity — and the local wound environment, where dead tissue, foreign material, haematoma, poor blood supply and dead space all favour bacterial growth. The Cruse and Foord concept captures this as infection risk being proportional to the dose of contamination multiplied by virulence and divided by host resistance: infection results when the bacterial challenge overcomes the host's defences in a permissive environment. The organisms responsible are a recognisable group: Staphylococcus aureus (including meticillin-resistant strains, MRSA) is the commonest cause of skin and surgical-site infection; streptococci typically cause spreading cellulitis; Escherichia coli and other coliforms and anaerobes such as Bacteroides dominate after gastrointestinal surgery; Clostridium species cause gas gangrene and tetanus; and Pseudomonas aeruginosa is an important cause in burns and in hospital-acquired infection. Understanding this balance is what makes infection preventable — every element on the host and environment side can be optimised, and every reduction in contamination tilts the balance toward healing.
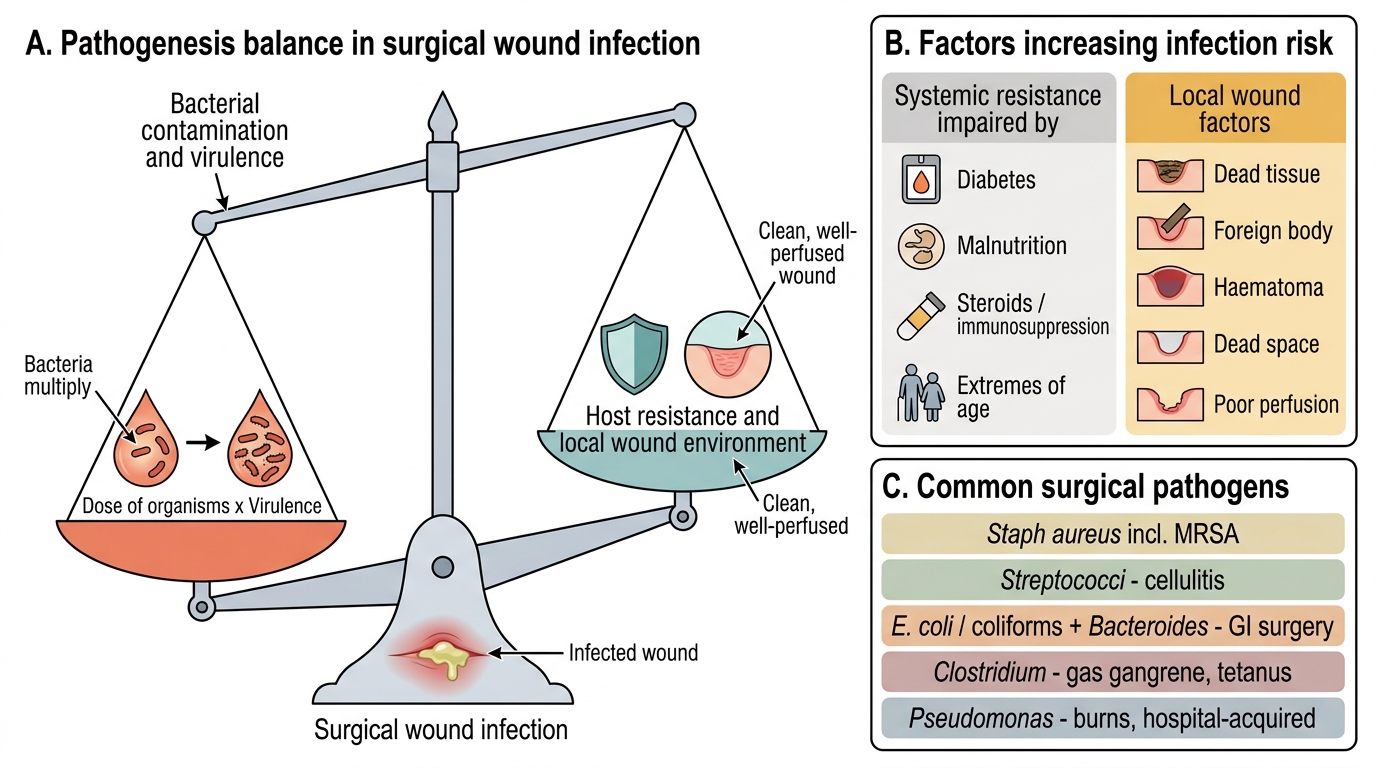
Pathogenesis of Surgical Wound Infection
- Pathogen side: dose (number) of organisms × their virulence.
- Host side: systemic resistance (impaired by diabetes, malnutrition, steroids/immunosuppression, age) and the local environment (dead tissue, foreign body, haematoma, dead space, poor perfusion).
- Common organisms: Staph aureus (incl. MRSA), streptococci (cellulitis), E. coli/coliforms and Bacteroides (after GI surgery), Clostridium (gas gangrene, tetanus), Pseudomonas (burns, hospital-acquired).
SELF-CHECK
Which single statement best captures the pathogenesis of surgical wound infection?
A. Infection occurs whenever any bacteria are present in a wound, regardless of other factors
B. Infection results when the dose and virulence of contaminating organisms overcome host resistance in a favourable local environment
C. Infection depends only on the patient's immune status and not on the wound itself
D. Infection is determined solely by whether prophylactic antibiotics were given
Reveal Answer
Answer: B. Infection results when the dose and virulence of contaminating organisms overcome host resistance in a favourable local environment
Infection is a balance: risk rises with the dose and virulence of contaminating organisms and falls with host resistance and a clean, well-perfused local environment (the Cruse-Foord concept). Mere presence of bacteria does not guarantee infection, and neither host nor wound factors act alone.
Types of Surgical Infection
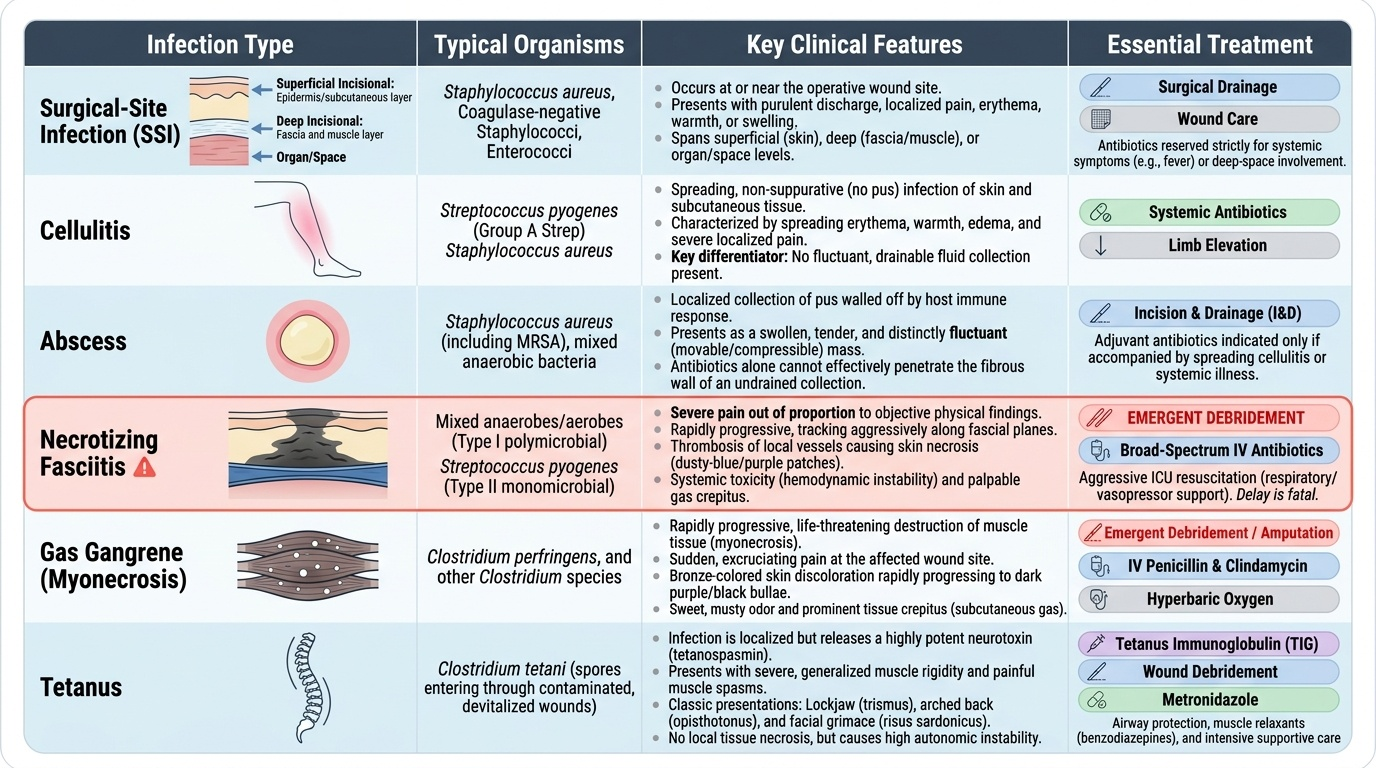
Surgical infections take several recognisable forms, and identifying which one is present directs treatment because the urgency and the operation differ sharply between them. A surgical-site infection (SSI) is infection at or near the operative wound and is subdivided, following the CDC, into superficial incisional (skin and subcutaneous tissue), deep incisional (fascia and muscle) and organ/space infection (a deeper structure or cavity opened or manipulated at operation, such as an intra-abdominal collection). Cellulitis is a spreading, non-suppurative infection of the skin and subcutaneous tissue, usually streptococcal, marked by spreading redness, warmth, swelling and pain without a drainable collection — it responds to antibiotics. An abscess is a localised collection of pus walled off by the body; it is fluctuant, and its essential treatment is drainage — antibiotics alone will not cure an undrained abscess. The most dangerous category is necrotizing fasciitis (a necrotizing soft-tissue infection), a rapidly spreading infection tracking along fascial planes with thrombosis of perforating vessels and necrosis; it causes pain out of proportion to the visible signs, systemic toxicity, skin changes and sometimes crepitus, and it is a surgical emergency requiring immediate, radical debridement plus broad-spectrum antibiotics and resuscitation — delay is fatal. Specific clostridial infections complete the picture: gas gangrene is myonecrosis caused by Clostridium perfringens, presenting with severe pain, crepitus and toxaemia and demanding urgent debridement; and tetanus, caused by Clostridium tetani, is prevented by the wound prophylaxis discussed earlier. The clinical rule is to recognise the suppurative, drainable and necrotizing forms quickly because each carries a different and time-critical surgical response.
Provided image
| Type | Typical organism | Key features | Essential treatment |
|---|---|---|---|
| Surgical-site infection | Staph aureus (incl. MRSA), coliforms | At/near wound; superficial, deep or organ/space | Open/drain if pus; antibiotics if cellulitic |
| Cellulitis | Streptococci | Spreading redness, warmth, swelling; no drainable pus | Antibiotics; elevate |
| Abscess | Staph aureus | Localised fluctuant pus collection | Drainage (incision and drainage) — antibiotics adjunctive |
| Necrotizing fasciitis | Mixed/Group A strep; surgical EMERGENCY | Pain out of proportion, toxicity, skin necrosis, ± crepitus | Immediate radical debridement + broad-spectrum antibiotics + resuscitation |
| Gas gangrene | Clostridium perfringens | Myonecrosis, severe pain, crepitus, toxaemia | Urgent debridement + antibiotics (± hyperbaric oxygen) |
| Tetanus | Clostridium tetani | Muscle spasm, trismus; from tetanus-prone wound | Prevention by wound prophylaxis; supportive care if established |