Page 5 of 14
SU5.3-4 | Wound Classification, Management and Medico-Legal Documentation — SDL Guide (Part 2)
Principles of Wound Management
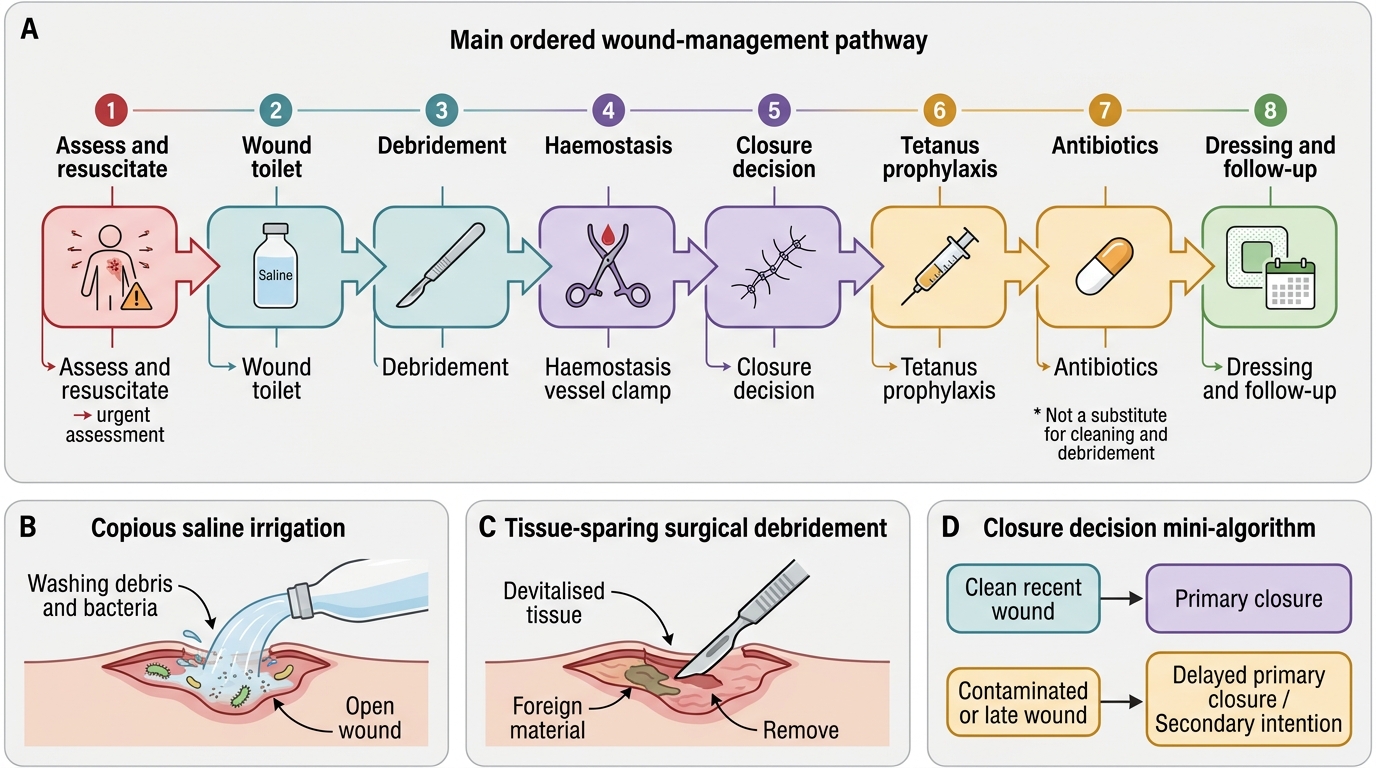
Wound management follows an ordered sequence of principles that applies, with adaptation, to almost any wound, and observing this order is what competency SU5.3 asks the student to plan and observe. First comes assessment and resuscitation as above, controlling life-threatening problems and haemorrhage before the wound itself. Next is wound toilet (cleaning) — copious irrigation with normal saline to wash out dirt, clot and loose contamination, the single most effective step in reducing wound bacterial load. This is followed by debridement, the surgical excision of all dead and devitalised tissue and the removal of any foreign material, since dead tissue and foreign bodies are the soil in which infection grows; debridement should be thorough but tissue-sparing. Haemostasis is then secured to prevent a haematoma, which is itself a culture medium. The pivotal decision is the type of closure: a clean, recent, well-perfused wound may be closed by primary suture; a contaminated wound, or one seen late, is better left open for delayed primary (tertiary) closure or allowed to heal by secondary intention. Tetanus prophylaxis is decided for every wound according to whether it is tetanus-prone (more than six hours old, more than one centimetre deep, contaminated with soil or faeces, containing devitalised tissue, or a puncture, missile or bite wound) and the patient's immunisation status — tetanus toxoid for boosting, with human tetanus immunoglobulin added for tetanus-prone wounds in the unimmunised or those of unknown status. Antibiotics are given as prophylaxis for clean-contaminated and contaminated wounds at risk, and therapeutically for established infection, but are never a substitute for cleaning and debridement. Finally an appropriate dressing is applied and a plan for follow-up, suture removal and rehabilitation is made.
Ordered Principles of Wound Management
- Assess and resuscitate: ATLS first; control haemorrhage before the wound.
- Wound toilet: copious saline irrigation — the most effective single step to cut bacterial load.
- Debridement: excise dead/devitalised tissue, remove foreign material; thorough but tissue-sparing.
- Haemostasis: prevent haematoma (a culture medium).
- Closure decision: primary for clean recent wounds; delayed primary/secondary for contaminated or late wounds.
- Tetanus prophylaxis: by wound type (tetanus-prone?) and immunisation status; toxoid ± human tetanus immunoglobulin.
- Antibiotics: prophylactic for at-risk contaminated wounds, therapeutic for infection — never a substitute for cleaning/debridement.
- Dressing and follow-up: appropriate dressing, planned review, suture removal, rehabilitation.
Medico-Legal Aspects of Wounds and Documentation
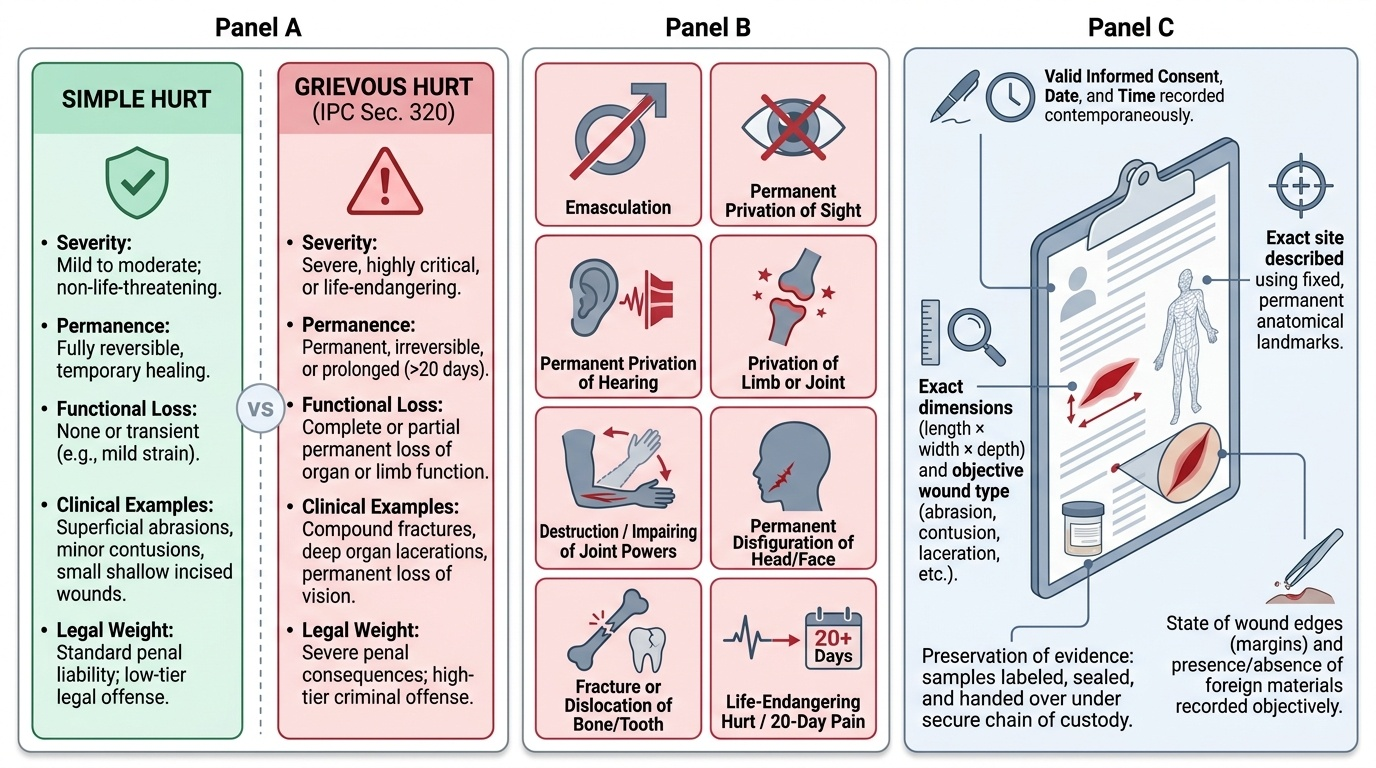
A wound is not only a clinical problem but, in law, an injury — and the doctor who treats it is frequently the person whose record decides a legal question, so competency SU5.4 requires the student to discuss these medico-legal aspects. The foundation is accurate, contemporaneous documentation: the wound's exact site (described from fixed anatomical landmarks), its dimensions, its type (incised, lacerated, abrasion, contusion and so on, described objectively rather than presumed cause), the state of its edges and surroundings, and the presence of foreign material — recorded factually, dated and timed, ideally with a diagram or photograph. The doctor should describe what is seen and avoid speculating about the weapon or the manner of causation beyond what the wound objectively shows. For medico-legal cases an injury report (often a medico-legal case or MLC document) is prepared, and in India injuries are categorised in law as simple or grievous hurt, the categories of grievous hurt being specifically enumerated in the Indian Penal Code (section 320 — for example fracture or dislocation of a bone, permanent loss of sight or hearing, or any hurt endangering life or causing the sufferer to be in severe bodily pain for twenty days). Valid informed consent must be obtained for examination and treatment, and the limits of confidentiality understood. Where the wound is evidence — for example in assault, sexual assault or firearm cases — preservation of evidence and chain of custody matters: clothing, foreign bodies and samples are retained, labelled and handed over correctly so that they remain admissible. Sound medico-legal practice protects the patient's interests, supports the administration of justice, and defends the treating doctor.
Provided image
Check Your Understanding
Before moving on, consolidate by reasoning through the three casualty patients from the start of this module rather than recalling isolated facts. The cook's palm wound is an incised wound — clean, sharp-edged, length exceeding depth; it is a recent, relatively clean wound, so after assessment (checking tendon and nerve function in the hand), wound toilet and haemostasis it can be closed by primary intention, with tetanus prophylaxis judged by his immunisation status. The motorcyclist's shin wound is a lacerated, dirt-ingrained, two-hour-old contaminated wound — a Class III wound that is tetanus-prone; it needs thorough irrigation and debridement, is best managed by delayed primary or secondary healing rather than immediate closure, and requires tetanus toxoid with immunoglobulin if he is unimmunised. The stab wound to the abdomen is a puncture wound whose small surface hides potential visceral injury — ATLS first, then exploration and imaging to exclude cavity penetration, and it is a medico-legal case demanding a careful injury report and preservation of evidence. Test yourself on three links: can you name a wound's morphological type and its contamination class; can you sequence its management from assessment to follow-up and justify the closure choice; and can you state its medico-legal handling? The questions below check exactly these.
CLINICAL PEARL
Two wounds look almost identical on the skin but mean very different things: a small, neat incised wound from a knife and a small puncture from a stab. The danger of the stab is depth — a one-centimetre surface wound over the chest or abdomen can have transfixed a great vessel or a hollow viscus. Never judge a penetrating wound by its surface; assume the track is as deep and as damaging as the instrument allows until exploration or imaging proves otherwise, and treat any such case as both a surgical emergency and a medico-legal one.
SELF-CHECK
Under Indian law, into which two categories is bodily injury (hurt) classified, with the more serious category — including fracture or dislocation of a bone and hurt endangering life — specifically enumerated in the Indian Penal Code?
A. Minor and major hurt
B. Simple and grievous hurt
C. Civil and criminal hurt
D. Primary and secondary hurt
Reveal Answer
Answer: B. Simple and grievous hurt
Indian law classifies hurt as simple or grievous; the categories of grievous hurt (including fracture or dislocation of a bone, permanent loss of sight or hearing, and any hurt endangering life) are specifically enumerated in section 320 of the Indian Penal Code. Accurate, objective wound documentation underpins this medico-legal categorisation.