Page 8 of 14
SU9.3 | Communicating Investigation Results — SDL Guide (Part 2)
Reading the Patient and the Consultation
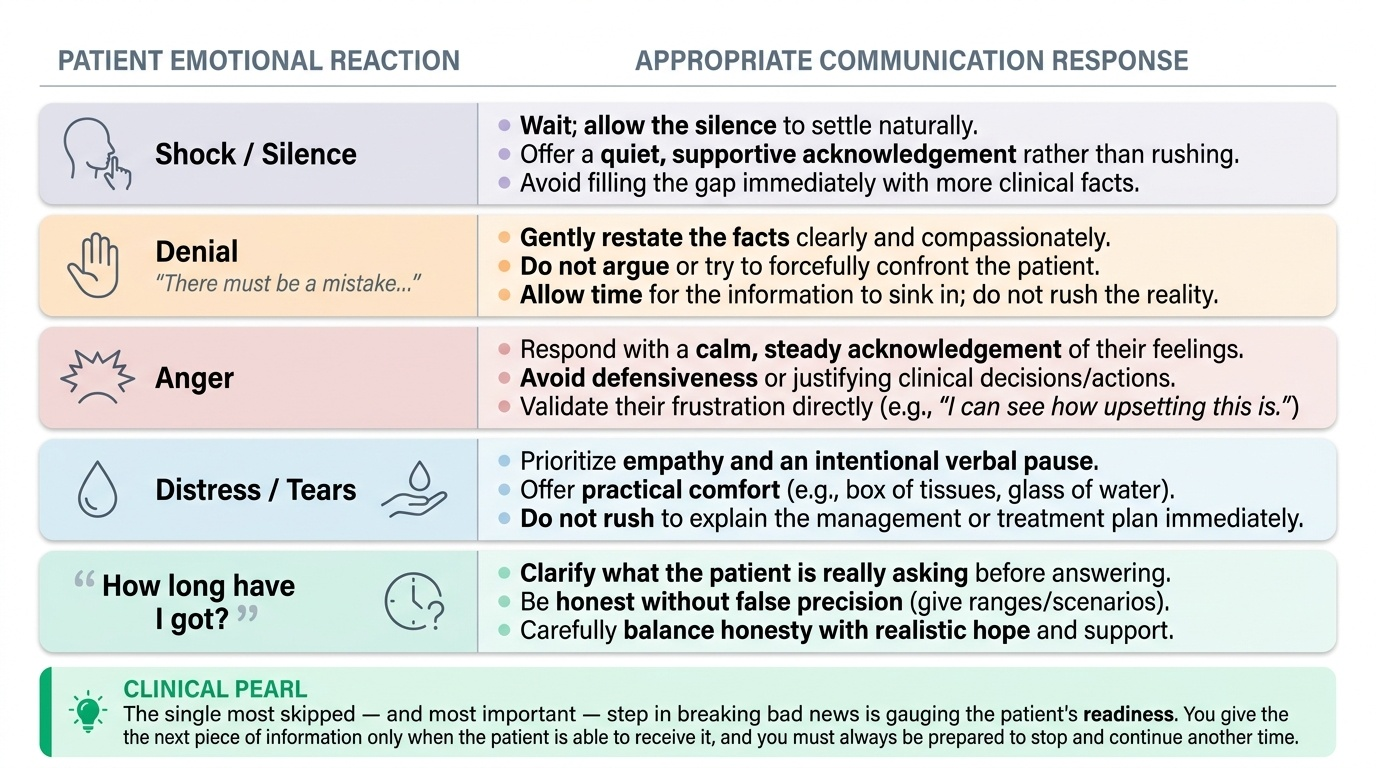
Delivering news is only half the skill; the other half is continuously reading the patient and adapting, because no protocol survives contact with real emotion unmodified. Throughout the conversation, attend to both verbal and non-verbal cues — facial expression, posture, tears, going quiet, sudden questions — and use them to judge whether to slow down, pause, or stop giving information altogether for the moment. Different reactions call for different responses, and recognising them is what the 'interpretation of findings' of this skill means. Shock or silence is common immediately after the news; the right response is to wait, to allow the silence, and to offer a quiet acknowledgement rather than filling the gap with more facts. Denial ('there must be a mistake') is a protective response; gently restate the facts without arguing, and allow time rather than confronting. Anger, sometimes directed at you, should be met with calm acknowledgement of the feeling rather than defensiveness. Overt distress or tears call for empathy, a pause, and practical comfort, not an immediate return to the management plan. Questions about prognosis ('how long have I got?') must be answered honestly but carefully — clarify what the patient is really asking, avoid false precision, and balance honesty with hope. The overarching judgement is one of readiness: you give the next piece of information only when the patient is able to receive it, and you are always prepared to stop and continue another time. Reading the patient well is what separates a checklist recital of SPIKES from genuine, compassionate communication.
Provided image
| Patient reaction | Appropriate response |
|---|---|
| Shock / silence | Wait; allow silence; quiet acknowledgement |
| Denial | Gently restate facts; do not argue; allow time |
| Anger | Calm acknowledgement of the feeling; not defensiveness |
| Distress / tears | Empathy, a pause, practical comfort before any plan |
| 'How long have I got?' | Clarify the real question; honest, no false precision; keep hope |
CLINICAL PEARL
The single most skipped — and most important — step in breaking bad news is responding to EMOTION before moving to the plan. A patient who has just heard 'cancer' is in shock and cannot take in chemotherapy schedules; if you press on, none of it is heard. Pause, name and acknowledge the emotion ('I can see this is a shock'), allow silence, and only move to strategy when the patient is ready. And always fire a warning shot before the news — 'I'm afraid it's serious' — so the diagnosis does not land out of nowhere.
Practising It: A Worked Consultation
Now walk through a complete consultation the way you will rehearse it in simulation. A 55-year-old woman returns for the result of a breast core biopsy that has shown carcinoma. Setting: you take her into a quiet room, sit down, ensure you will not be interrupted, and offer to have her husband present; she accepts. Perception: you ask what she has been told and what she is worried about — she says she knows the lump was being checked and fears it could be 'something bad'. Invitation: you ask whether she would like to know the full results today; she says yes, she wants to understand everything. Knowledge: you give a warning shot — 'I'm afraid the biopsy result is more serious than we hoped' — pause, and then, in plain language and small chunks, explain that it has shown a breast cancer, checking she is following. Emotions: she becomes tearful and falls silent; you stop, acknowledge — 'I can see this is a real shock' — pass tissues, allow the silence, and wait until she is ready rather than ploughing on. Strategy and Summary: when she can engage, you explain the next steps clearly — that her case will go to the multidisciplinary team, that further staging investigations are needed, and that you will discuss the treatment options (which may include surgery, with oncology input) together once the team has met; you mention the breast-care nurse and written information, summarise, and check her understanding with teach-back, asking her to tell you in her own words what will happen next. You confirm a follow-up appointment and a contact number. Rehearsing the whole arc — setting, ask-before-tell, warning shot, chunked plain-language news, empathic pause, and a clear plan with checked understanding — under supervision is exactly the applied practice this competency demands.
Check Your Understanding
Consolidate the skill as a repeatable approach you can run in any result conversation. Hold the principles steady whatever the news: protect confidentiality and consent, speak in plain language and small chunks, start from what the patient knows and wants, be honest without being brutal, check understanding with teach-back, and respond to emotion before problem-solving. For serious news, run the SPIKES structure in order — Setting, Perception (ask before you tell), Invitation, Knowledge (warning shot, then chunked plain language), Emotions (empathy and silence), Strategy and summary (agree the plan, including multidisciplinary review and support, and re-check understanding). Throughout, read the patient — shock, denial, anger, distress, prognosis questions each call for a different response — and gauge readiness before giving the next piece of information. End every serious conversation with a clear next step, named support and follow-up. Self-test on four links: can you list the six SPIKES steps and say what each does; can you explain why you respond to emotion before giving the plan; can you describe an appropriate response to denial or to 'how long have I got?'; and can you state the principles that apply to any result, good or bad? The questions below check exactly these.
SELF-CHECK
A patient who has just been told she has cancer becomes tearful and silent. According to good bad-news practice (and the SPIKES 'E' step), what is the most appropriate immediate response?
A. Quickly move on to explain the full chemotherapy and surgery plan so she has hope
B. Acknowledge the emotion empathically, allow silence, and wait until she is ready before continuing
C. Tell her not to cry because the prognosis might be good
D. End the consultation immediately and reschedule for another doctor
Reveal Answer
Answer: B. Acknowledge the emotion empathically, allow silence, and wait until she is ready before continuing
The Emotions step requires you to respond to the patient's emotion FIRST — name and acknowledge it, allow silence, and wait until she is ready before moving on. A shocked patient cannot absorb a management plan, so pressing on with treatment detail (or dismissing her feelings, or abruptly ending the encounter) is wrong; empathy precedes problem-solving.