Page 13 of 20
SU17.8-10 | Chest Injury Assessment and Emergency Management — SDL Guide
Learning Objectives
- Describe the pathophysiology of chest injuries and how they impair oxygenation, ventilation and circulation (SU17.8).
- Describe the clinical features and the principles of management of chest injuries (SU17.9).
- Demonstrate airway maintenance and the recognition and management of tension pneumothorax, haemothorax and flail chest in a simulated environment (SU17.10).
INSTRUCTIONS
Chest trauma is responsible for a large share of trauma deaths, yet most of those deaths are preventable with simple, immediate bedside actions — a needle, a chest drain, a dressing — that any trained doctor can perform. The thorax houses the lungs, heart and great vessels, so an injury here strikes directly at oxygenation and circulation, and a handful of conditions can kill within minutes if not recognised in the first examination. This module teaches you the pathophysiology of chest injury, how to recognise the immediately life-threatening problems at the bedside, and the emergency manoeuvres — airway control, needle decompression, chest drain and dressings — that you will rehearse in simulation.
References
- Bailey & Love's Short Practice of Surgery, Cardiothoracic Trauma (textbook)
- SRB's Manual of Surgery, Chest Injuries (textbook)
- Advanced Trauma Life Support (ATLS) Student Course Manual, American College of Surgeons — Thoracic Trauma (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young man is wheeled into casualty after a road crash, fighting for breath. He is restless and frightened, his lips are turning blue, and his blood pressure is falling fast. As you watch, the veins in his neck stand out, his trachea looks pushed to one side, and one half of his chest is barely moving and sounds hollow when you tap it. There is no time for an X-ray and no time to wait — this man has air trapped under pressure in his chest, squeezing his lung flat and throttling the great veins returning blood to his heart, and he will be dead in minutes unless someone releases that pressure with a needle right now. Chest trauma is unusual in surgery precisely because of moments like this: the diagnosis is made at the bedside, the treatment is immediate and simple, and the difference between life and death is whether the doctor recognised the pattern and acted without hesitation.
WHY THIS MATTERS
Chest injuries cause a quarter of all trauma deaths, and they are common in a country with heavy road and industrial trauma. What makes them so important for every doctor — not just thoracic surgeons — is that the great majority are managed without major surgery: roughly eighty-five per cent need only airway control, oxygen and a chest drain, all of which a general doctor can provide. Conversely, the conditions that kill quickly — tension pneumothorax, massive haemothorax, cardiac tamponade — are recognised and treated at the bedside in the first minutes, long before any specialist arrives. Getting this right saves lives that no later operation could; missing it loses them. As a graduate you are expected to recognise the immediately life-threatening chest injuries, maintain an airway, and perform or assist needle decompression and chest-drain insertion. These are demonstrated and assessed in simulation, because hesitation or error in a real tension pneumothorax is fatal.
RECALL
Recall the anatomy and physiology that explain chest trauma. From AN: each lung sits in its pleural space, the chest wall is supported by the ribs and moved by the intercostal and other muscles, and the heart lies in the pericardium between the lungs, with the great veins returning blood to it. Recall the safe triangle for chest-drain insertion — bordered by the lateral edge of pectoralis major, the anterior border of latissimus dorsi and a line at the level of the nipple (around the fifth intercostal space, anterior to the mid-axillary line) — chosen to avoid the heart, great vessels, liver and spleen. From PY: normal breathing depends on a negative intrapleural pressure that keeps the lung expanded, so air or blood entering the pleural space collapses the lung; and the heart fills during diastole only if blood can return to it, so anything that compresses the great veins or the heart impairs venous return and therefore cardiac output. Hold on to these two ideas — collapse of the lung and obstruction of venous return — because together they explain how every life-threatening chest injury kills.
The Patient with a Chest Injury
Chest (thoracic) trauma presents as some combination of respiratory distress and circulatory compromise, because the injured thorax interferes directly with breathing and with the heart's filling. The mechanism may be blunt (road crashes, falls, assaults — causing rib fractures, lung contusions and, by deceleration, great-vessel injury) or penetrating (stabs and gunshots — causing pneumothorax, haemothorax and direct cardiac injury). Clinically, the patient may show breathlessness, rapid shallow breathing, chest pain worsened by breathing, cyanosis, reduced or absent breath sounds on one side, surgical emphysema (air crackling under the skin), a flail (paradoxically moving) chest segment, distended neck veins, hypotension and shock. The clinician's first job is to identify the immediately life-threatening injuries — the small group of conditions that kill within minutes and are sought during the primary survey: tension pneumothorax, open pneumothorax, massive haemothorax, flail chest with pulmonary contusion, and cardiac tamponade. These are distinguished from the potentially life-threatening injuries found on fuller assessment (simple pneumothorax/haemothorax, pulmonary contusion, tracheobronchial, aortic, diaphragmatic and oesophageal injuries) and from minor injuries such as isolated rib fractures. The defining clinical lesson of chest trauma is that recognition is rapid and bedside-based: the most lethal injuries are diagnosed by looking, feeling, percussing and listening to the chest in the first minute, not by waiting for imaging.
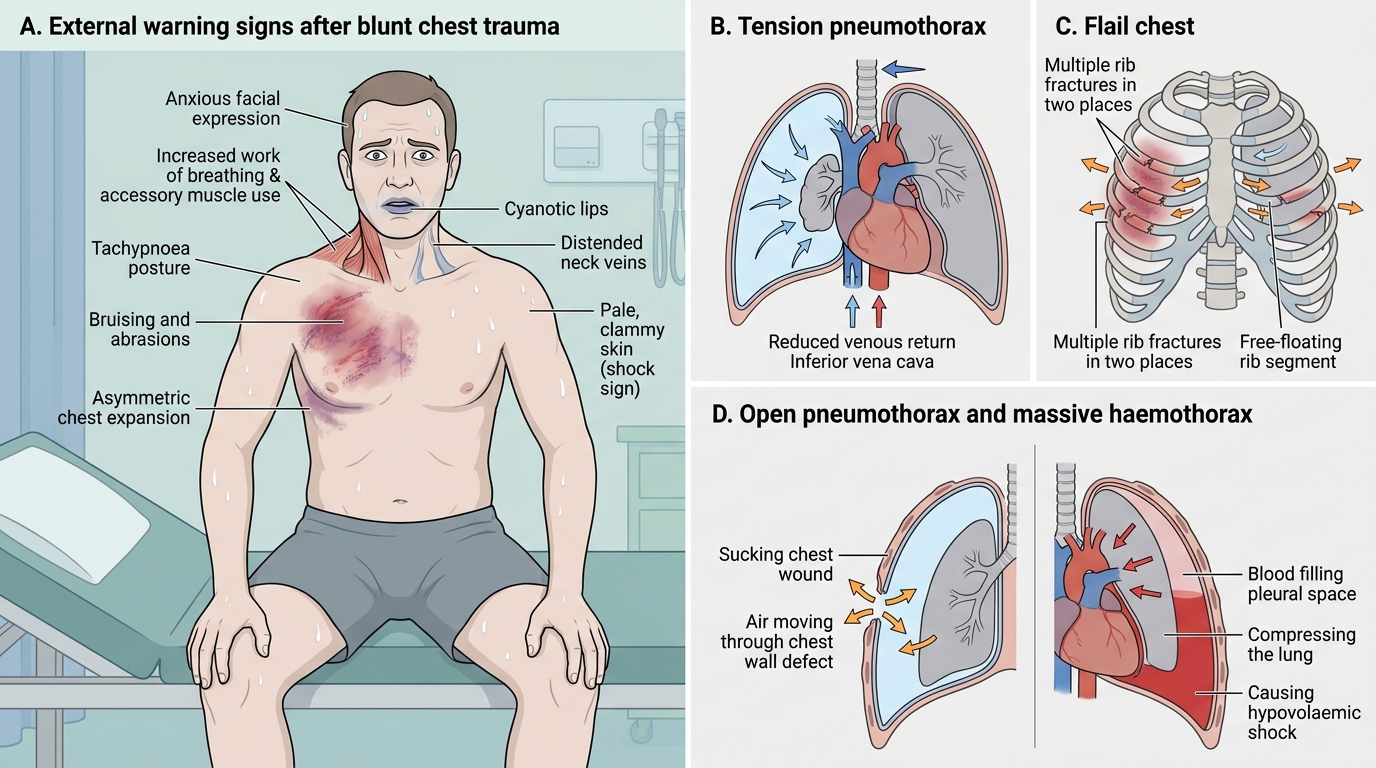
Blunt Chest Trauma: External Signs of Life-Threatening Thoracic Injury
Pathophysiology of Thoracic Trauma
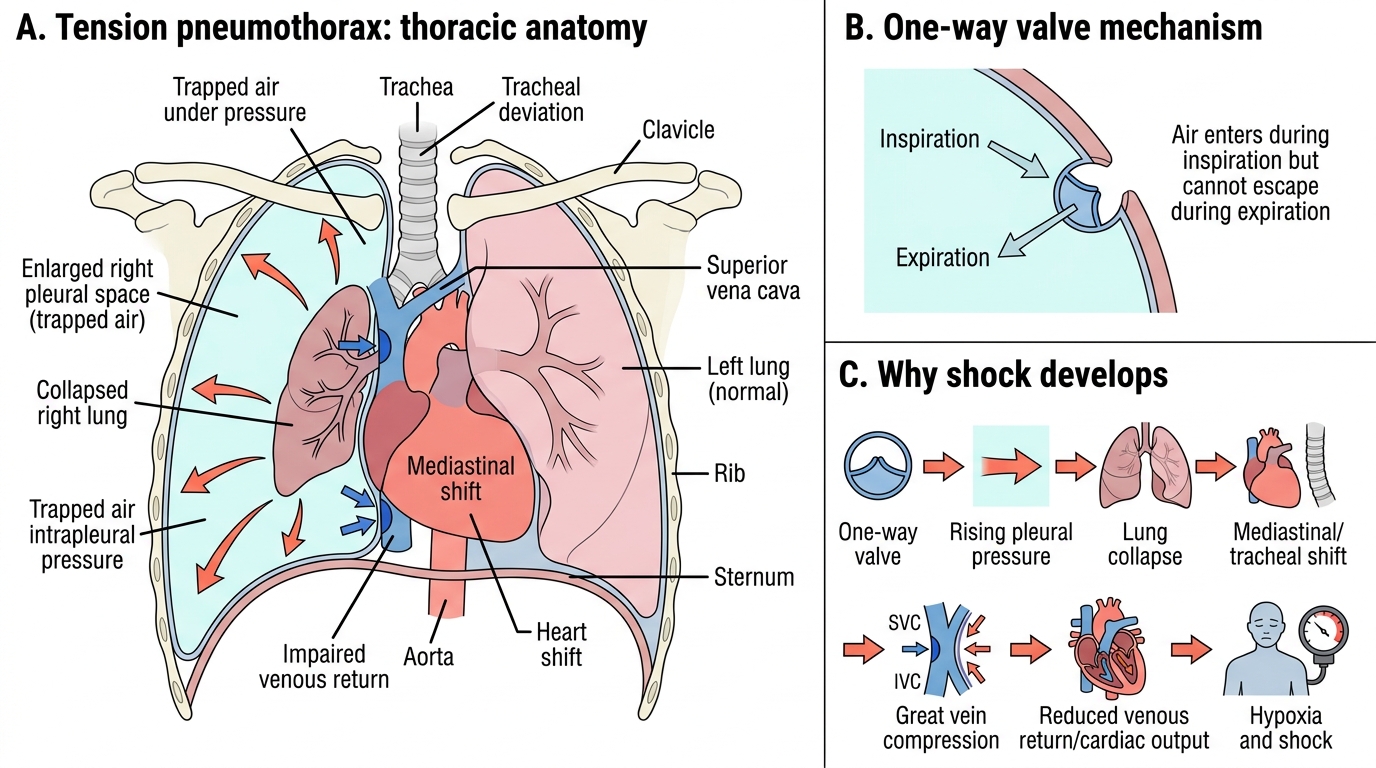
Chest injuries kill by three overlapping mechanisms — hypoxia, impaired ventilation, and impaired venous return/cardiac output — and each life-threatening condition can be understood through them. A tension pneumothorax occurs when a chest-wall or lung injury acts as a one-way valve, letting air enter the pleural space with each breath but not escape; the trapped air builds up under increasing pressure, collapsing the lung (hypoxia), pushing the mediastinum and trachea to the opposite side, and crucially compressing the great veins so that venous return — and thus cardiac output — falls, producing rapidly worsening shock. This combination of respiratory and circulatory collapse is why it kills so fast. An open pneumothorax (sucking chest wound) is a chest-wall defect through which air moves preferentially in and out of the pleural space rather than the trachea, impairing ventilation. A massive haemothorax is rapid bleeding into the pleural space (from lung, intercostal or great vessels) that both compresses the lung (hypoxia) and causes major blood loss (hypovolaemic shock). A flail chest results when a segment of chest wall is detached by fractures of two or more adjacent ribs each broken in two or more places; this free segment moves paradoxically (in on inspiration, out on expiration), impairing ventilation, but the chief danger is the underlying pulmonary contusion that causes hypoxia. Cardiac tamponade is blood accumulating in the pericardium, which compresses the heart and prevents it filling in diastole — directly impairing cardiac output. Understanding these mechanisms tells you exactly what each emergency treatment must reverse: release trapped air, seal the wound, drain blood and restore volume, support ventilation, and relieve the pericardium.
Tension Pneumothorax: Lung Collapse, Mediastinal Shift, and Shock
- Three killing mechanisms: hypoxia, impaired ventilation, impaired venous return/cardiac output.
- Tension pneumothorax: one-way valve → rising pressure → lung collapse + mediastinal shift + impaired venous return.
- Open pneumothorax: chest-wall defect → air moves in/out of pleura instead of trachea → poor ventilation.
- Massive haemothorax: pleural bleeding → lung compression + hypovolaemic shock.
- Flail chest: free segment, paradoxical movement; the real danger is the underlying pulmonary contusion.
- Cardiac tamponade: pericardial blood → heart cannot fill → falling cardiac output.
SELF-CHECK
Why does a tension pneumothorax cause rapidly progressive shock as well as breathlessness?
A. It causes massive blood loss into the chest
B. Trapped air under pressure shifts the mediastinum and compresses the great veins, reducing venous return and cardiac output
C. It floods the pericardium with blood
D. It directly stops the heart from beating
Reveal Answer
Answer: B. Trapped air under pressure shifts the mediastinum and compresses the great veins, reducing venous return and cardiac output
In a tension pneumothorax, a one-way valve traps air under rising pressure, collapsing the lung (hypoxia) AND shifting the mediastinum to compress the great veins, so venous return and therefore cardiac output fall — causing shock. The blood-loss mechanism describes massive haemothorax; pericardial blood describes tamponade.
Recognising the Life-Threatening Injuries — Examination and Investigation
Recognition of the immediately life-threatening chest injuries is a clinical skill performed during the primary survey, and for the most lethal of them treatment must not wait for any investigation. A tension pneumothorax is a clinical diagnosis: severe respiratory distress and shock, absent breath sounds and a hyper-resonant (hollow) percussion note on the affected side, distended neck veins, and a trachea deviated to the opposite side — recognising this pattern mandates immediate treatment without waiting for a chest X-ray, because the delay can be fatal. An open pneumothorax is recognised by a visible sucking chest wound through which air bubbles with breathing. A massive haemothorax presents with respiratory distress and the signs of shock combined with absent breath sounds but a dull (stony) percussion note on the affected side (blood, not air) and flat neck veins from blood loss. A flail chest is recognised by inspecting and palpating a chest-wall segment that moves paradoxically with breathing, with crepitus over the fractured ribs and a hypoxic patient. Cardiac tamponade is recognised by Beck's triad — muffled (distant) heart sounds, distended neck veins (raised JVP) and hypotension — in a patient (often with penetrating precordial injury) who is in shock despite no obvious blood loss; it can be confirmed rapidly at the bedside by ultrasound. Once the immediate threats are excluded or treated, investigations characterise the rest: a chest X-ray (CXR) shows pneumothorax, haemothorax, rib fractures and a widened mediastinum; eFAST ultrasound rapidly detects pericardial fluid and pneumo-/haemothorax; arterial blood gases gauge oxygenation and ventilation; and CT is reserved for the stable patient to define lung, mediastinal and aortic injury. The discipline is simple: treat the killers on clinical signs first, image second.
Provided image
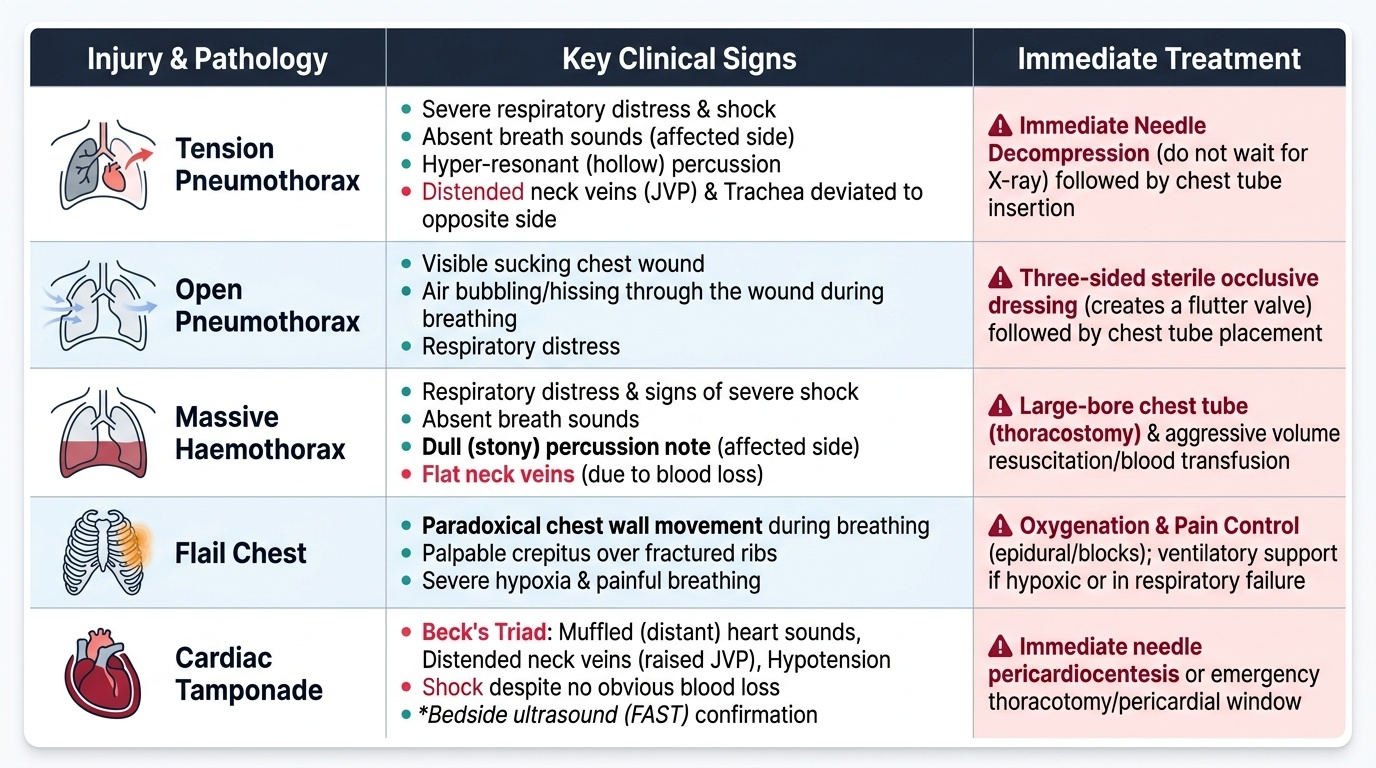
| Injury | Key clinical signs | Immediate treatment |
|---|---|---|
| Tension pneumothorax | Distress + shock, absent breath sounds, hyper-resonant, trachea deviated AWAY, distended neck veins | Immediate needle decompression then chest drain (ICD) — no X-ray first |
| Open pneumothorax | Sucking chest wound, air bubbling | Three-sided occlusive dressing then chest drain |
| Massive haemothorax | Shock, absent breath sounds, dull percussion, flat neck veins | Chest drain + volume/blood; thoracotomy if >1500 mL or >200 mL/h |
| Flail chest | Paradoxical chest-wall movement, crepitus, hypoxia | Oxygen, analgesia, ventilatory support; treat pulmonary contusion |
| Cardiac tamponade | Beck's triad: muffled heart sounds + raised JVP + hypotension | Pericardiocentesis / emergency thoracotomy |