Page 14 of 20
SU17.8-10 | Chest Injury Assessment and Emergency Management — SDL Guide (Part 2)
Emergency Management — Airway, the Primary-Survey Injuries and the Chest Drain
The emergency management of chest trauma follows the ATLS primary survey (ABCDE), treating each life-threatening injury the moment it is found rather than completing the survey first. Airway is secured with cervical-spine control, ensuring it is patent and giving high-flow oxygen — airway maintenance is the first demonstrated skill and the foundation of all that follows. Breathing is then assessed and the breathing-related killers treated at once: a tension pneumothorax is relieved by immediate needle decompression (a wide-bore cannula inserted into the pleural space to release the trapped air — historically the second intercostal space in the mid-clavicular line, with the fifth intercostal space anterior to the mid-axillary line now also recommended), which is always followed by a definitive intercostal chest drain (ICD) placed in the safe triangle and connected to an underwater seal. An open pneumothorax is covered with a three-sided occlusive dressing (which lets air escape on expiration but prevents entry on inspiration, averting a tension) and then a chest drain placed away from the wound. A flail chest is managed with oxygen, good analgesia and chest physiotherapy, with positive-pressure ventilation if respiratory failure develops — and the underlying pulmonary contusion is treated, while excessive fluid is avoided. Circulation is addressed next: a massive haemothorax is treated by restoring volume with blood and inserting a large chest drain; an immediate drainage of more than 1500 mL, or continued bleeding of more than 200 mL per hour, is the indication for thoracotomy. Cardiac tamponade is relieved by pericardiocentesis or emergency thoracotomy. The reassuring principle is that the majority of chest injuries (~85%) are managed without thoracotomy — by airway control, oxygen and a chest drain alone — so the skills you rehearse in simulation (airway maintenance, needle decompression, the three-sided dressing, and chest-drain insertion into the safe triangle) cover most of what actually saves these patients.
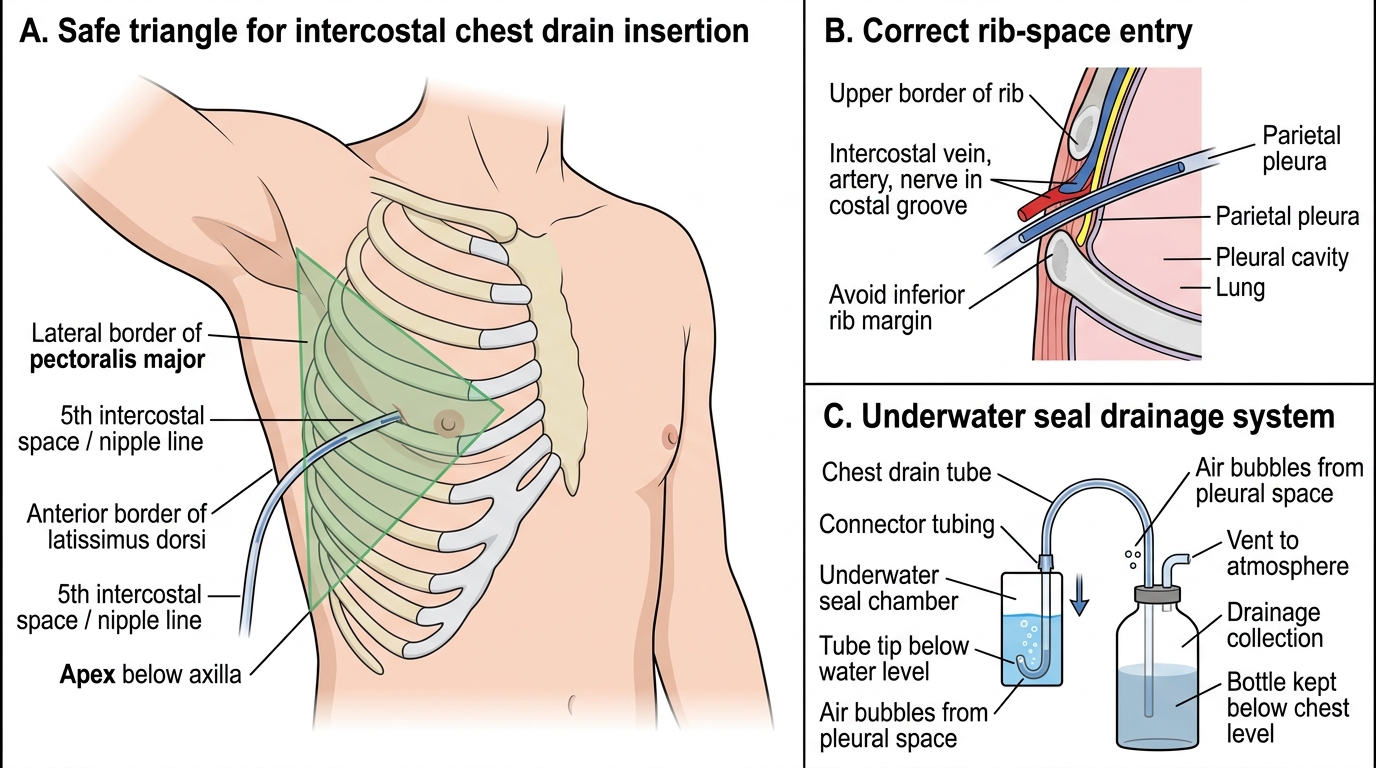
Intercostal Chest Drain in the Safe Triangle
- Airway: patent airway + C-spine control + high-flow oxygen (first skill).
- Tension pneumothorax: immediate needle decompression → definitive intercostal chest drain (safe triangle, underwater seal); never wait for X-ray.
- Open pneumothorax: three-sided occlusive dressing → chest drain.
- Flail chest: oxygen, analgesia, physiotherapy, ventilation if needed; treat pulmonary contusion.
- Massive haemothorax: chest drain + blood; thoracotomy if >1500 mL or >200 mL/h.
- Cardiac tamponade: pericardiocentesis / thoracotomy.
- ~85% need no thoracotomy — airway, oxygen and a chest drain manage most.
CLINICAL PEARL
A tension pneumothorax is diagnosed with your eyes and hands, NOT with an X-ray — and treated with a needle, immediately. If you see a shocked, breathless patient with absent breath sounds, a hyper-resonant chest and deviated trachea, decompress at once; sending them to the X-ray department first can kill them. Two quick discriminators help at the bedside: a tension pneumothorax is hyper-resonant (air) while a massive haemothorax is stony dull (blood), and cardiac tamponade gives Beck's triad — muffled heart sounds, raised JVP and hypotension — in a shocked patient with no obvious external blood loss. Remember too that most chest injuries are saved not by heroic surgery but by a chest drain placed correctly in the safe triangle.
Check Your Understanding
Return to the breathless crash victim from the hook and reason through him. His severe distress and shock, absent breath sounds with a hyper-resonant chest, distended neck veins and a trachea deviated to the opposite side are the unmistakable picture of a tension pneumothorax — a one-way valve trapping air under pressure that has collapsed his lung and, by shifting the mediastinum and compressing the great veins, is throttling his venous return and causing shock. The pathophysiology dictates the treatment: this is a clinical diagnosis demanding immediate needle decompression without an X-ray, followed by a definitive intercostal chest drain in the safe triangle. Contrast him with the alternatives you must distinguish: had his chest been stony dull with flat neck veins, you would have suspected a massive haemothorax (drain, blood, and thoracotomy if >1500 mL or >200 mL/h); had he shown Beck's triad of muffled heart sounds, raised JVP and hypotension, you would have suspected cardiac tamponade; and a paradoxically moving chest-wall segment would point to a flail chest with pulmonary contusion. Throughout, airway maintenance with oxygen comes first. Self-test on four links: can you explain the three mechanisms by which chest injuries kill; can you list the five immediately life-threatening injuries and the bedside signs of each; can you state the immediate treatment of tension pneumothorax, open pneumothorax, massive haemothorax, flail chest and tamponade; and can you give the thoracotomy thresholds for haemothorax? The questions in this module check exactly these.
SELF-CHECK
A trauma patient has a chest drain inserted for a haemothorax. Which finding is the accepted indication for urgent thoracotomy?
A. Any blood at all in the chest drain
B. Initial drainage of 300 mL
C. Initial drainage of more than 1500 mL, or ongoing loss of more than 200 mL per hour
D. A residual small pneumothorax on the follow-up X-ray
Reveal Answer
Answer: C. Initial drainage of more than 1500 mL, or ongoing loss of more than 200 mL per hour
A massive haemothorax — an immediate drainage of more than 1500 mL of blood, or continued bleeding of more than 200 mL per hour (typically over 2-4 hours) — is the indication for thoracotomy. Smaller volumes are usually managed by the chest drain alone, as most chest injuries do not require thoracotomy.