Page 1 of 20
SU17.1-2 | First Aid, Basic Life Support and Transport — SDL Guide
Learning Objectives
- Describe the principles of first aid — its aims, scene safety and the primary assessment of a casualty (SU17.1).
- Demonstrate the steps of adult Basic Life Support, including high-quality chest compressions and the use of an automated external defibrillator (SU17.2).
- Demonstrate the recovery position and the safe transport of an injured patient with spinal precautions in a simulated environment (SU17.2).
INSTRUCTIONS
Most deaths after trauma or sudden collapse that are preventable are decided in the first few minutes, long before the patient reaches a hospital. First aid and Basic Life Support are the skills that bridge that gap — simple, sequenced, hands-on actions that any trained person can deliver at the roadside to keep a casualty alive until definitive care arrives. This module gives you the principles of first aid, the exact sequence of adult Basic Life Support, and the technique of moving an injured patient safely, all of which you will rehearse in simulation until they are automatic.
References
- Bailey & Love's Short Practice of Surgery, Trauma and the Early Management of the Injured (textbook)
- SRB's Manual of Surgery, First Aid and Basic Life Support (textbook)
- Advanced Trauma Life Support (ATLS) Student Course Manual, American College of Surgeons (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are walking out of college when a motorcyclist a few metres ahead is struck by a car. He is thrown onto the road and lies still. A crowd gathers, phones come out, but no one moves towards him. For the next several minutes — until an ambulance can possibly arrive — whatever happens to this man depends entirely on whoever steps forward. If his airway is blocked by his own tongue or by blood, he will suffocate. If his heart has stopped, every minute without chest compressions roughly halves his chance of survival. None of the help he needs in these minutes requires a hospital, a drug or a machine; it requires a trained pair of hands acting in the right order. That trained pair of hands could be yours, and this module is about exactly what you would do.
WHY THIS MATTERS
First aid and Basic Life Support are the most widely useful clinical skills you will ever learn, because the situations that need them happen everywhere — homes, roads, wards and public places — and almost always before any doctor or equipment is present. The principle behind the trauma 'golden hour' is that early, correct, simple interventions decide outcome; a cleared airway, effective chest compressions and safe movement of an injured spine prevent deaths that no later surgery can reverse. As a clinician you will also be expected to lead a resuscitation, teach these skills to others, and supervise the safe transfer of patients between departments and facilities. Just as importantly, these are competencies you can use as a citizen the moment you finish this session, which is why they are demonstrated and assessed in simulation before anything else in trauma care.
RECALL
Recall the physiology that makes these minutes so unforgiving. From PY and AN: the brain depends on a continuous supply of oxygenated blood and begins to suffer irreversible injury within only a few minutes of arrest, which is why circulation must be restored fast. Recall that in an unconscious person lying supine the commonest cause of airway obstruction is the tongue falling back against the posterior pharyngeal wall, relieved by simple airway-opening manoeuvres. Recall too the concept of agonal breathing — the occasional, gasping, ineffective breaths that may follow a cardiac arrest and which must NOT be mistaken for normal breathing. Hold on to one parallel: inside the hospital, the structured trauma assessment is the ATLS primary survey (ABCDE); the roadside first-aider version you will learn here is a streamlined sequence built on the same logic — find and fix the immediately fatal problems first.
When You Are First on the Scene
The clinical indication for first aid is any situation where a person is injured or suddenly taken ill and definitive medical care is not yet available — which, for the most time-critical emergencies, is the rule rather than the exception. First aid is the immediate assistance given to a casualty before professional help arrives, and the first-aider is whoever provides it. The value of the role is entirely about time: in cardiac arrest, survival falls with every minute that compressions and defibrillation are delayed, and in major trauma the early control of airway, breathing and bleeding determines whether the patient survives long enough to benefit from hospital care — the reasoning behind the golden hour. Three aims define everything a first-aider does, and they are worth committing to memory because they resolve almost every dilemma at a scene: to preserve life, to prevent the condition from worsening, and to promote recovery. Before any of this, however, comes a rule that overrides them all: ensure your own safety first. A rescuer who becomes a second casualty — struck by traffic, electrocuted, overcome by fumes — helps no one and adds to the burden. So the first action at every scene is to assess danger to yourself, the casualty and bystanders, make the area safe where you can, and only then approach. This single discipline of 'safe approach before action' is what separates effective help from well-meaning harm.
Principles of First Aid and the Primary Assessment
With the scene made safe, first aid proceeds by a fixed primary assessment that finds and treats immediately life-threatening problems in the order in which they kill. The widely taught sequence is DRSABC: Danger (confirm the scene is safe), Response (check whether the casualty responds to voice and to a gentle shake of the shoulders), Shout for help (call out for bystanders and activate the emergency medical services — in India dial 108 / 112), then Airway, Breathing and Circulation. The logic is that an obstructed airway kills in minutes, absent breathing kills next, and catastrophic circulatory failure (arrest or massive bleeding) kills after that — so each is checked and corrected before moving on. If the casualty responds and is breathing normally, you reassess, treat injuries and keep them comfortable; if the casualty is unresponsive and not breathing normally, this is a cardiac arrest until proven otherwise and you move immediately into Basic Life Support. Throughout, the first-aider also controls obvious severe external bleeding with direct pressure, protects a possibly injured spine by avoiding unnecessary movement, keeps the casualty warm, and gives nothing by mouth. Calling for help early matters as much as the hands-on care: defibrillation and ambulance transport must be set in motion at the start, not after several minutes of effort, because the first-aider's job is to keep the casualty alive until that help arrives.
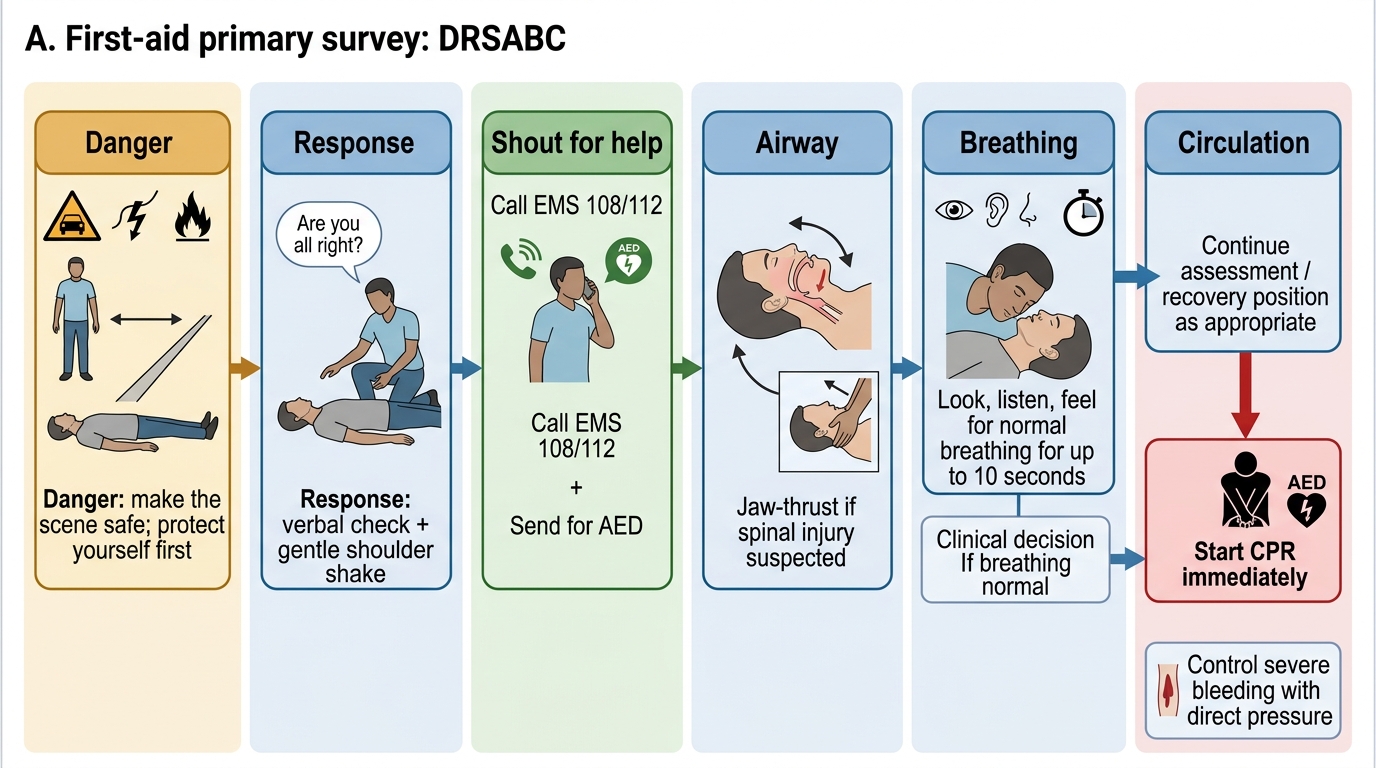
First-Aid Primary Survey: DRSABC Sequence
- D — Danger: make the scene safe; protect yourself first.
- R — Response: 'Are you all right?' + gentle shoulder shake.
- S — Shout for help: call bystanders; activate EMS (108/112); send for an AED.
- A — Airway: open the airway (head-tilt/chin-lift; jaw-thrust if spinal injury suspected).
- B — Breathing: look, listen and feel for normal breathing for up to 10 seconds.
- C — Circulation: if not breathing normally → start CPR; control severe bleeding with direct pressure.
SELF-CHECK
You arrive at the side of a collapsed adult. According to the principles of first aid, what is the very FIRST thing you must do before touching the casualty?
A. Start chest compressions immediately
B. Check whether the scene is safe for you and the casualty
C. Open the airway with a head-tilt, chin-lift
D. Place the casualty in the recovery position
Reveal Answer
Answer: B. Check whether the scene is safe for you and the casualty
The overriding first principle is rescuer safety — assess Danger before approaching, because a rescuer who becomes a second casualty helps no one. Only once the scene is safe do you check Response, shout for help, and then assess Airway, Breathing and Circulation.
Performing Adult Basic Life Support
Basic Life Support is the hands-on technique that keeps oxygenated blood moving to the brain and heart when an adult's circulation has stopped, and it is performed in a precise sequence you must be able to demonstrate without hesitation. Having confirmed the scene is safe, check responsiveness by shaking the shoulders and shouting; if there is no response, shout for help, activate EMS and send someone for an AED. Open the airway with a head-tilt and chin-lift (use a jaw-thrust if a cervical-spine injury is suspected) and, for no more than 10 seconds, look, listen and feel for normal breathing. If the casualty is not breathing or is only gasping (agonal breathing), begin chest compressions at once — the modern adult sequence is C-A-B (Circulation first) so that compressions are not delayed. Place the heel of one hand in the centre of the chest (lower half of the sternum), the other hand on top, and push hard and fast: at a rate of 100-120 compressions per minute, to a depth of 5-6 cm, allowing the chest to recoil fully between compressions and keeping interruptions to under 10 seconds. After every 30 compressions, if trained and willing, give 2 rescue breaths — the adult ratio is 30:2 — each breath delivered over about one second and just enough to make the chest rise; if unable or unwilling to give breaths, continuous compression-only CPR is acceptable and far better than nothing. As soon as an AED (automated external defibrillator) arrives, switch it on and follow its voice prompts: it analyses the rhythm and advises a shock only for shockable rhythms (ventricular fibrillation or pulseless ventricular tachycardia), never for asystole. Continue cycles of CPR, swapping the compressor every two minutes to avoid fatigue, until the casualty shows signs of life, a defibrillator/EMS team takes over, or you are exhausted.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
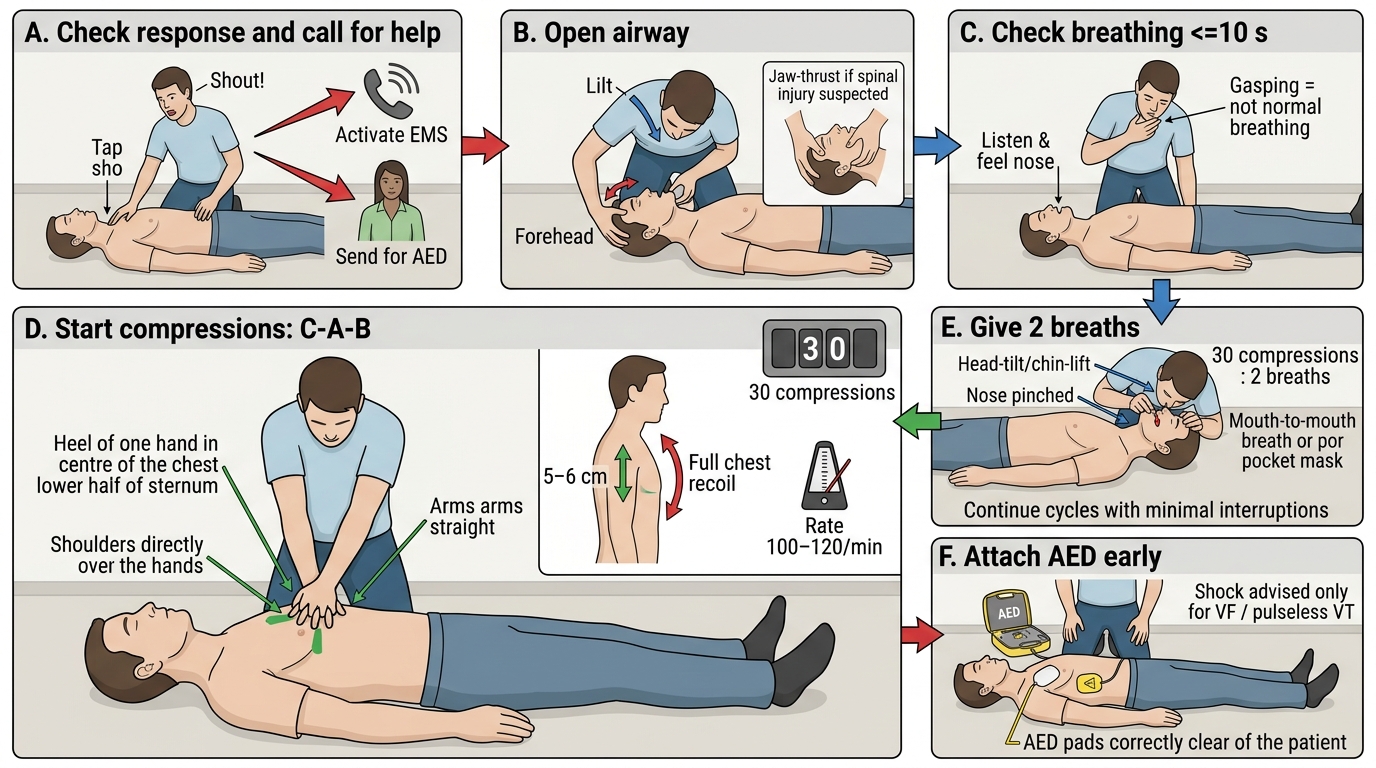
Adult Basic Life Support Sequence
- Check response → shout for help, activate EMS, send for AED.
- Airway: head-tilt/chin-lift (jaw-thrust if spinal injury suspected).
- Breathing: look/listen/feel ≤10 s; gasping = NOT normal breathing.
- Compressions (start first, C-A-B): centre of chest, rate 100-120/min, depth 5-6 cm, full recoil, minimal interruptions.
- Ratio: 30 compressions : 2 breaths (compression-only acceptable if untrained/unwilling to ventilate).
- AED: attach early; shock advised only for VF/pulseless VT.