Page 2 of 20
SU17.1-2 | First Aid, Basic Life Support and Transport — SDL Guide (Part 2)
Reading the Casualty — Signs of Effective and Failing Resuscitation
Performing the steps is not enough; the rescuer must continuously read the casualty to know whether resuscitation is working and what to do next. The most important judgement is made at the very start — distinguishing normal breathing from agonal gasping. Agonal breaths are slow, irregular, gasping or snoring efforts that commonly appear in the first minutes after cardiac arrest; mistaking them for normal breathing is a classic and fatal error, so any breathing that is not regular and effective should be treated as no breathing and CPR started. During CPR, judge the quality of compressions against the targets — correct rate (100-120/min), adequate depth (5-6 cm) and full recoil — because shallow, slow or non-recoiling compressions perfuse poorly; this is why feedback and two-minute rescuer changes matter. Watch for signs of return of spontaneous circulation (ROSC): the casualty starts to move, cough, open the eyes or breathe normally. Only when normal breathing clearly returns do you stop compressions and reassess. When the AED analyses the rhythm, understand what its advice means: a 'shock advised' message indicates a shockable rhythm (VF or pulseless VT) and you must ensure no one is touching the casualty before the shock is delivered; a 'no shock advised' message means a non-shockable rhythm (asystole or PEA) and you resume compressions immediately rather than assuming the casualty is beyond help. Finally, if the casualty is unresponsive but breathing normally — for example after recovering, or in a non-arrest collapse — the correct action is not CPR but the recovery position, which protects the airway while you await transport.
SELF-CHECK
While giving adult CPR, what are the correct rate and depth of chest compressions?
A. Rate 60-80 per minute, depth 2-3 cm
B. Rate 100-120 per minute, depth 5-6 cm
C. Rate 140-160 per minute, depth 7-8 cm
D. Rate as fast as possible, depth until you feel a rib give way
Reveal Answer
Answer: B. Rate 100-120 per minute, depth 5-6 cm
High-quality adult chest compressions are delivered at a rate of 100-120 per minute to a depth of 5-6 cm (at least 5, not more than 6), with full chest recoil between compressions and minimal interruptions. Too slow or too shallow fails to perfuse the brain and heart; the compression:ventilation ratio is 30:2.
Recovery Position and Safe Transport of the Injured
Once a casualty is breathing but cannot protect their own airway, or once they must be moved, the first-aider's task shifts to protecting the airway and the spine during positioning and transport — skills you will rehearse under supervision in simulation. An unresponsive casualty who is breathing normally and has no suspected spinal injury should be placed in the recovery position: rolled onto their side with the head tilted slightly back and the upper leg and arm positioned to keep them stable, so that the tongue cannot fall back and any vomit or secretions drain out of the mouth rather than into the airway. Where a spinal injury is suspected — any significant trauma, a fall from height, a road traffic crash, or any unconscious trauma victim — the priority changes: keep the head, neck and trunk aligned in one straight line and avoid all unnecessary movement. If such a patient must be turned (for example to clear the airway of vomit) or moved onto a stretcher, use a coordinated log-roll: several rescuers turn the patient as a single rigid unit while one person holds the head in manual in-line immobilisation, maintaining the alignment of the spine throughout. For transport, immobilise the whole patient — a cervical collar and a rigid spine board or scoop stretcher for suspected spinal injury, and splinting of obviously fractured limbs to reduce pain, bleeding and further soft-tissue damage. Splint a limb in the position found, padding bony prominences and immobilising the joint above and below the fracture, and check the circulation and sensation distal to the splint before and after applying it. Throughout transfer, keep the casualty warm, keep monitoring airway and breathing, and hand over a clear account to the receiving team.
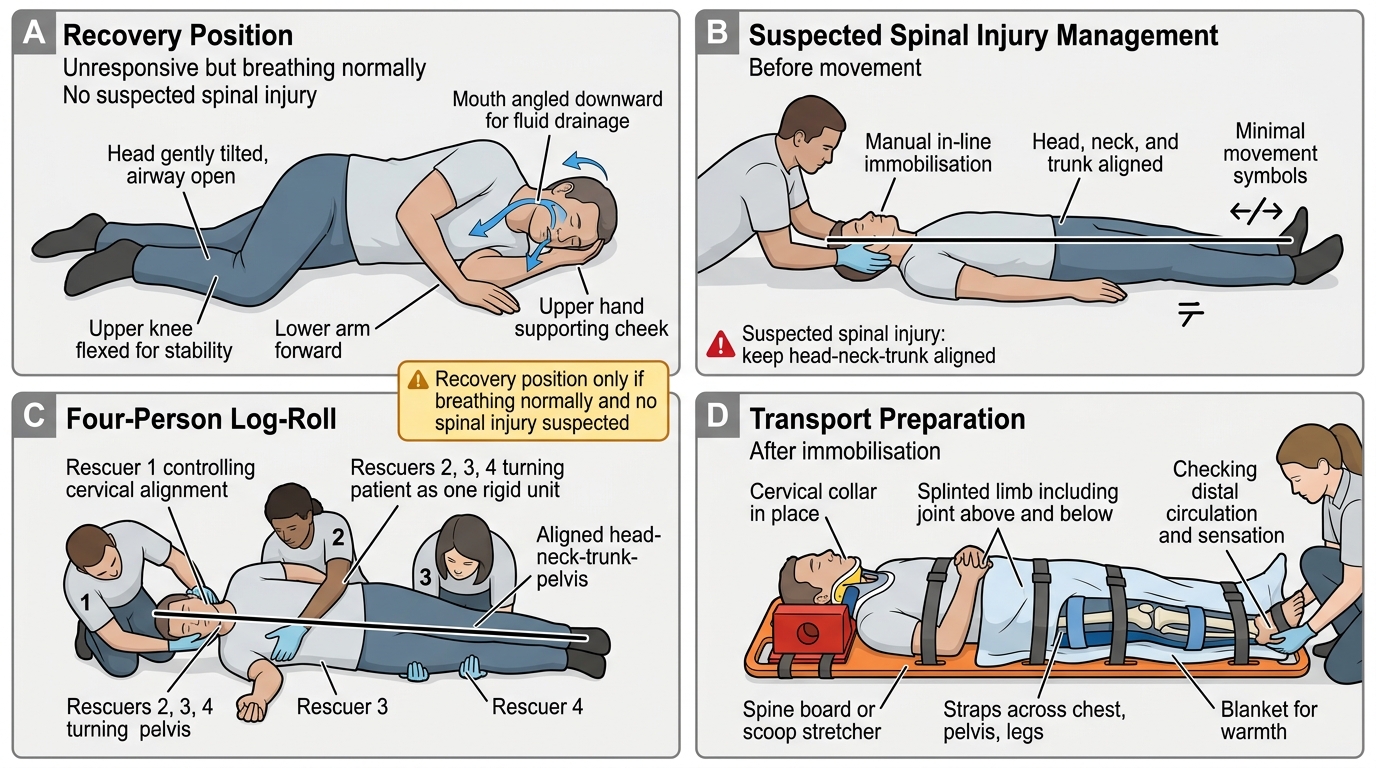
Recovery Position and Spinal Log-Roll Immobilisation
- Recovery position: unresponsive but breathing, NO suspected spinal injury — side-lying, airway protected, secretions drain out.
- Suspected spinal injury: keep head-neck-trunk aligned; minimise movement; manual in-line immobilisation.
- Log-roll: turn the patient as one rigid unit, one rescuer controlling the head.
- Transport: cervical collar + spine board/scoop stretcher; splint fractures (joint above and below), check distal circulation/sensation; keep warm; reassess airway and breathing.
CLINICAL PEARL
Do not be fooled by gasping. In the first minutes after a cardiac arrest, the casualty may take occasional slow, noisy, gasping breaths — agonal breathing — and a panicked bystander often reports 'he's still breathing' and withholds CPR. Agonal gasps are a sign of arrest, NOT of life: if an unresponsive adult is not breathing normally, start chest compressions immediately. Equally, never delay compressions to hunt for a pulse — for the first-aider, 'unresponsive and not breathing normally' is enough to begin.
Check Your Understanding
Bring the whole sequence together by replaying the injured motorcyclist from the hook. Your first action is not to touch him but to check for danger — oncoming traffic — and make the scene safe; only then do you check his response, shout for help and activate EMS (108/112) and call for an AED, and assess his airway and breathing. If he is unresponsive and not breathing normally — remembering that gasps do not count — you start chest compressions in the centre of the chest at 100-120 per minute, 5-6 cm deep, in cycles of 30 compressions to 2 breaths, attaching the AED as soon as it arrives and shocking only if it advises a shockable rhythm. If instead he is unresponsive but breathing, and you have no concern about his spine, you use the recovery position; but because this is a high-energy road crash you must assume a spinal injury, keep his head, neck and trunk aligned, and move him only by a coordinated log-roll with manual in-line immobilisation, splinting any obvious limb fracture before transport. Self-test on four links: can you state the three aims of first aid and the DRSABC sequence; can you recite the adult BLS rate, depth and ratio from memory; can you explain why agonal breathing must trigger CPR; and can you describe when to use the recovery position versus full spinal precautions? The questions across this module check exactly these.