Page 1 of 20
SU27.1-2 | Occlusive Arterial Disease — SDL Guide
Learning Objectives
- Describe the etiopathogenesis, clinical features, investigations and principles of treatment of occlusive arterial disease (SU27.1).
- Demonstrate the correct examination of the peripheral arterial system and enumerate and describe the investigation of vascular disease, including the ankle-brachial pressure index (SU27.2).
INSTRUCTIONS
A leg that hurts on walking, or a foot that has turned cold, pale and pulseless, is telling you that an artery has narrowed or blocked. Occlusive arterial disease runs along a single spectrum — from the cramping calf pain of intermittent claudication, through pain at rest, to tissue loss and gangrene — and the surgeon's task is to recognise where on that spectrum a patient sits, distinguish a slowly narrowing artery from a suddenly occluded one, and act with the right urgency. This module connects the pathology of atherosclerosis and Buerger's disease to a disciplined vascular examination, the bedside ankle-brachial index, and the principles that decide between risk-factor control, revascularisation and, when the limb cannot be saved, amputation.
References
- Bailey & Love's Short Practice of Surgery, Arterial Disorders (textbook)
- SRB's Manual of Surgery, Arterial Diseases (textbook)
- Sabiston Textbook of Surgery, Peripheral Arterial Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 62-year-old man who has smoked for forty years complains that for the past year his right calf cramps and forces him to stop after walking about a hundred metres; a minute's rest eases it and he walks on. Lately the distance has shrunk, and now his forefoot aches at night, easing only when he hangs it out of bed. In the next cubicle lies a 70-year-old woman in atrial fibrillation whose left leg became suddenly painful, white and numb three hours ago; you cannot feel any pulse below her groin and the foot is cold. Two patients, two tempos — one a slowly tightening artery you have weeks to plan for, the other a blocked artery that will cost the limb within hours unless you act now. Telling these apart, quickly and correctly, is the whole of this topic.
WHY THIS MATTERS
Occlusive arterial disease is common, disabling and, when acute, limb- and life-threatening — and most of the decisions that matter are made at the bedside before any scan. Peripheral arterial disease is a marker of generalised atherosclerosis, so the same patient is at high risk of myocardial infarction and stroke; recognising it is a chance to prevent a cardiovascular death, not just to save a leg. The acute, painful, pulseless limb is one of the few true vascular emergencies a junior doctor must recognise instantly, because the window to restore flow is measured in hours. As a final-year student you are expected to perform a clean peripheral arterial examination, measure and interpret an ankle-brachial pressure index, and state when a limb needs urgent revascularisation rather than reassurance. These are examined skills and, more importantly, skills that change outcomes.
RECALL
Recall the foundations this builds on. From anatomy: the lower-limb arterial tree runs from the external iliac to the common femoral artery at the groin, into the superficial femoral artery down the thigh, through the adductor (Hunter's) canal to become the popliteal artery behind the knee, which divides into the anterior tibial (continuing as dorsalis pedis on the foot) and the tibioperoneal trunk giving the posterior tibial (behind the medial malleolus) and peroneal arteries — these are the pulses you will palpate. From pathology: atherosclerosis begins with endothelial injury and lipid-laden plaque in large and medium arteries, and a plaque can narrow a vessel slowly or rupture and thrombose suddenly. Hold on to one physiological idea — ischaemia is a mismatch between oxygen supply and demand, so a narrowing that is silent at rest declares itself first on exercise (claudication) and only later at rest, as the disease worsens.
The Patient with the Painful, Pulseless Leg
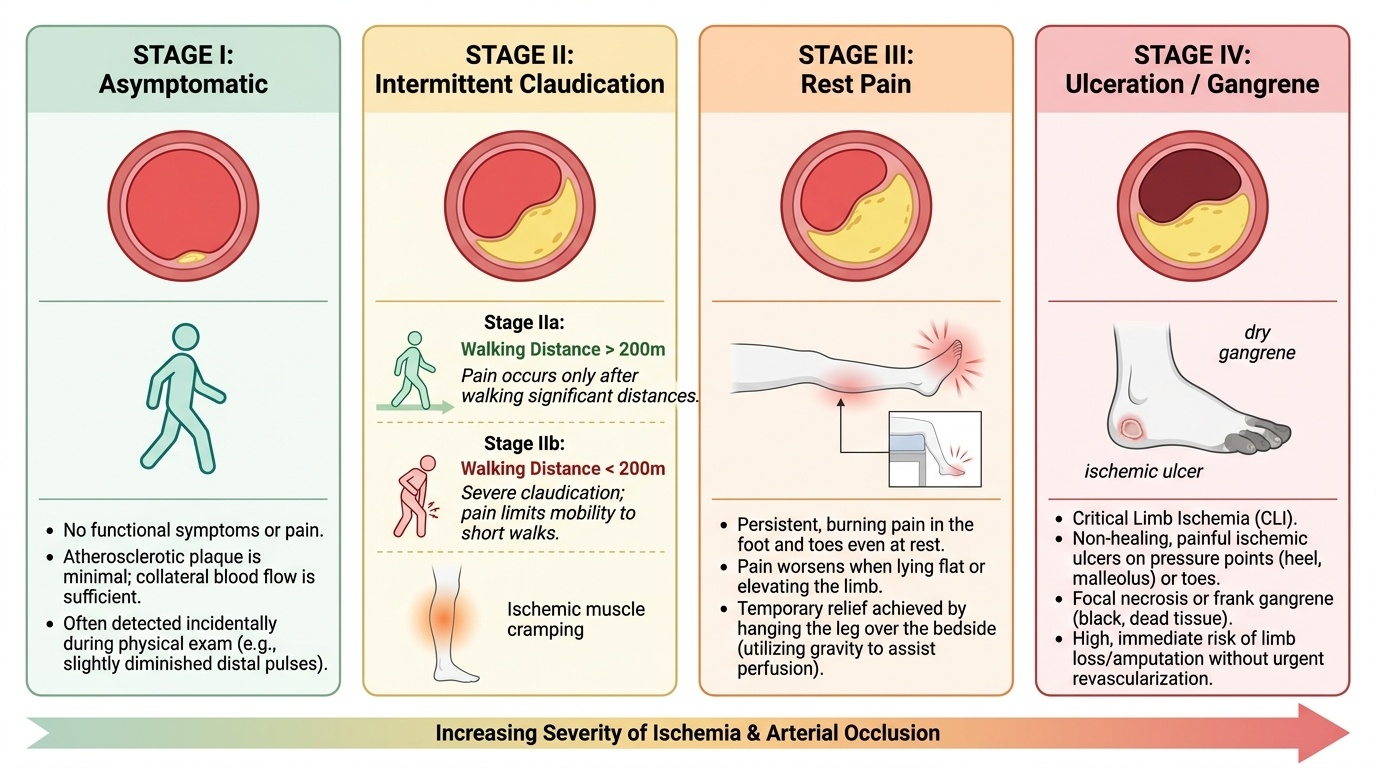
Occlusive arterial disease presents along one continuous clinical spectrum, and your first job is to place the patient on it. The mildest stage is intermittent claudication: a cramping, aching pain in a muscle group (classically the calf, but the buttock or thigh if the disease is higher up) brought on by walking a reproducible distance and relieved within a few minutes of rest — the muscle outruns its blood supply on exercise and recovers when demand falls. As disease progresses the patient develops rest pain: a severe, burning pain in the forefoot and toes, worst at night when the leg is horizontal, characteristically relieved by hanging the foot over the edge of the bed (gravity helps perfusion). The end of the chronic spectrum is tissue loss — ulceration or gangrene of the toes, heel or foot — and the combination of rest pain for more than two weeks and/or tissue loss defines critical (chronic) limb-threatening ischaemia, which carries a high risk of limb loss without revascularisation. Running parallel to this slow story is the surgical emergency of acute limb ischaemia, where an artery occludes suddenly (by embolus or in-situ thrombosis) and the limb declares itself within hours through the six P's — Pain, Pallor, Pulselessness, Paraesthesia, Paralysis and Perishing cold (a cold limb). The later P's, paraesthesia and paralysis, signal nerve and muscle death and mean the limb is in immediate jeopardy. Throughout, ask about smoking, diabetes, hypertension, hyperlipidaemia and ischaemic heart disease, because the leg is a window onto the whole arterial tree.
Pathology and the Vascular Basis of Ischaemia
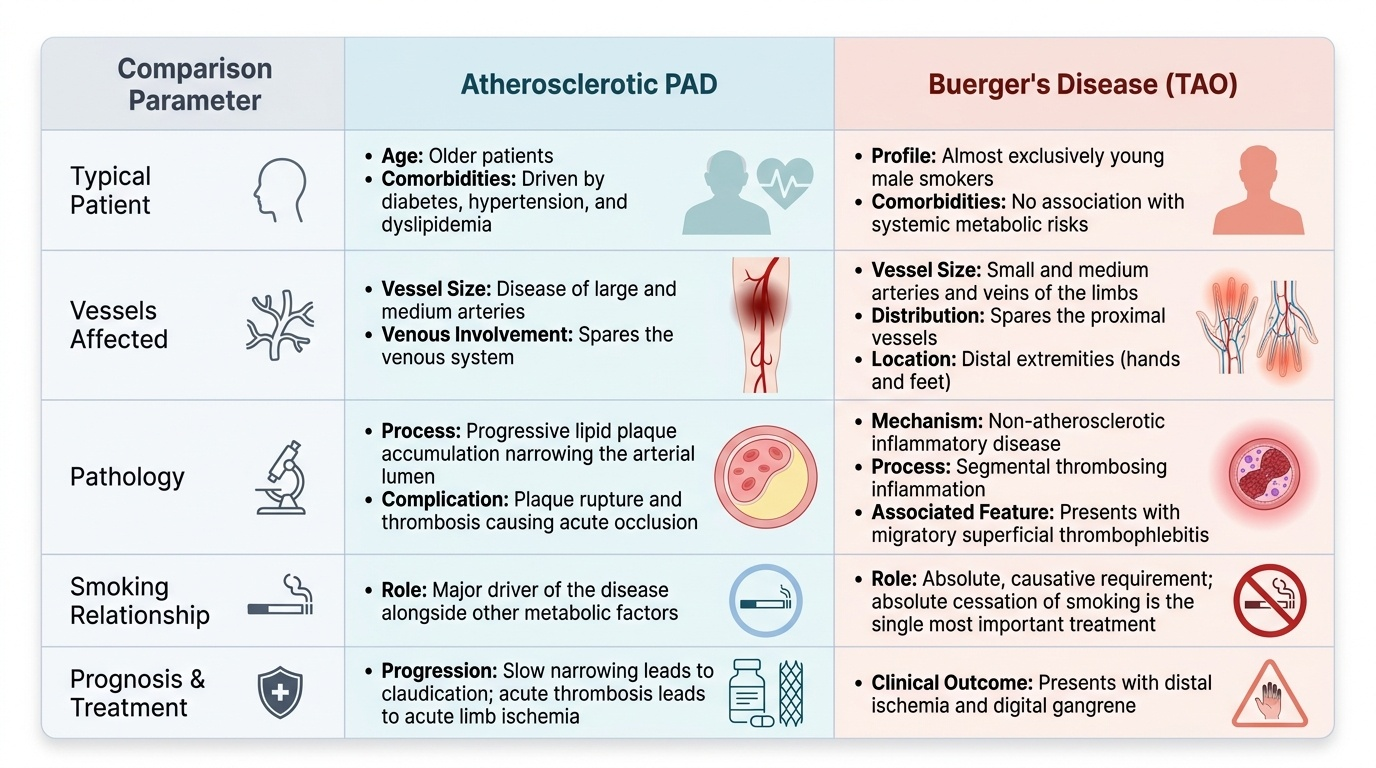
Ischaemia results when arterial inflow fails to meet tissue oxygen demand, and the two diseases that cause this in the limb have quite different biology. Atherosclerosis is overwhelmingly the commonest cause: a disease of large and medium arteries in older patients driven by smoking, diabetes, hypertension and dyslipidaemia, in which lipid plaques progressively narrow the lumen (giving claudication) and can rupture and thrombose to cause acute occlusion. Thromboangiitis obliterans (Buerger's disease) is a quite separate, non-atherosclerotic inflammatory disease: a segmental thrombosing inflammation of the small and medium arteries and veins of the limbs, occurring almost exclusively in young male smokers, sparing the proximal vessels and presenting with distal ischaemia, migratory superficial thrombophlebitis and digital gangrene — its single most important treatment is absolute cessation of smoking. The severity of chronic ischaemia is graded to standardise communication and decisions: the Fontaine classification runs I (asymptomatic), IIa (claudication on walking more than 200 m), IIb (claudication under 200 m), III (rest pain) to IV (ulceration or gangrene); the Rutherford classification grades the same spectrum in categories 0–6. Acute limb ischaemia is mechanistically different again: an embolus (commonly from the fibrillating left atrium or a mural thrombus after myocardial infarction) lodges at an arterial bifurcation in an otherwise healthy vessel, whereas in-situ thrombosis occurs on pre-existing atherosclerotic disease — a distinction that influences the operation chosen.
Provided image
Provided image
- Atherosclerosis: commonest; large/medium arteries; older smokers, diabetics; slow narrowing or acute thrombosis.
- Buerger's disease (TAO): young male smokers; small/medium distal vessels; inflammatory thrombosis; smoking cessation is paramount.
- Fontaine I–IV: asymptomatic → claudication (IIa >200 m, IIb <200 m) → rest pain → ulceration/gangrene.
- Acute ischaemia: embolic (healthy vessel, AF/post-MI) vs thrombotic (diseased vessel).
SELF-CHECK
A 30-year-old man who smokes heavily presents with painful ischaemia of the toes and migratory superficial thrombophlebitis, with normal proximal pulses. Which diagnosis and which single intervention matter most?
A. Atherosclerosis; start a statin
B. Buerger's disease (thromboangiitis obliterans); complete smoking cessation
C. Acute embolic ischaemia; urgent embolectomy
D. Raynaud's disease; calcium-channel blocker
Reveal Answer
Answer: B. Buerger's disease (thromboangiitis obliterans); complete smoking cessation
A young male smoker with distal small-vessel ischaemia, digital gangrene and migratory thrombophlebitis is the classic picture of Buerger's disease (thromboangiitis obliterans). The disease is inflammatory and non-atherosclerotic, affects small and medium distal vessels, and the single most effective treatment is absolute and complete cessation of smoking — no revascularisation succeeds if the patient keeps smoking.
Examining the Vascular System and Investigating Ischaemia
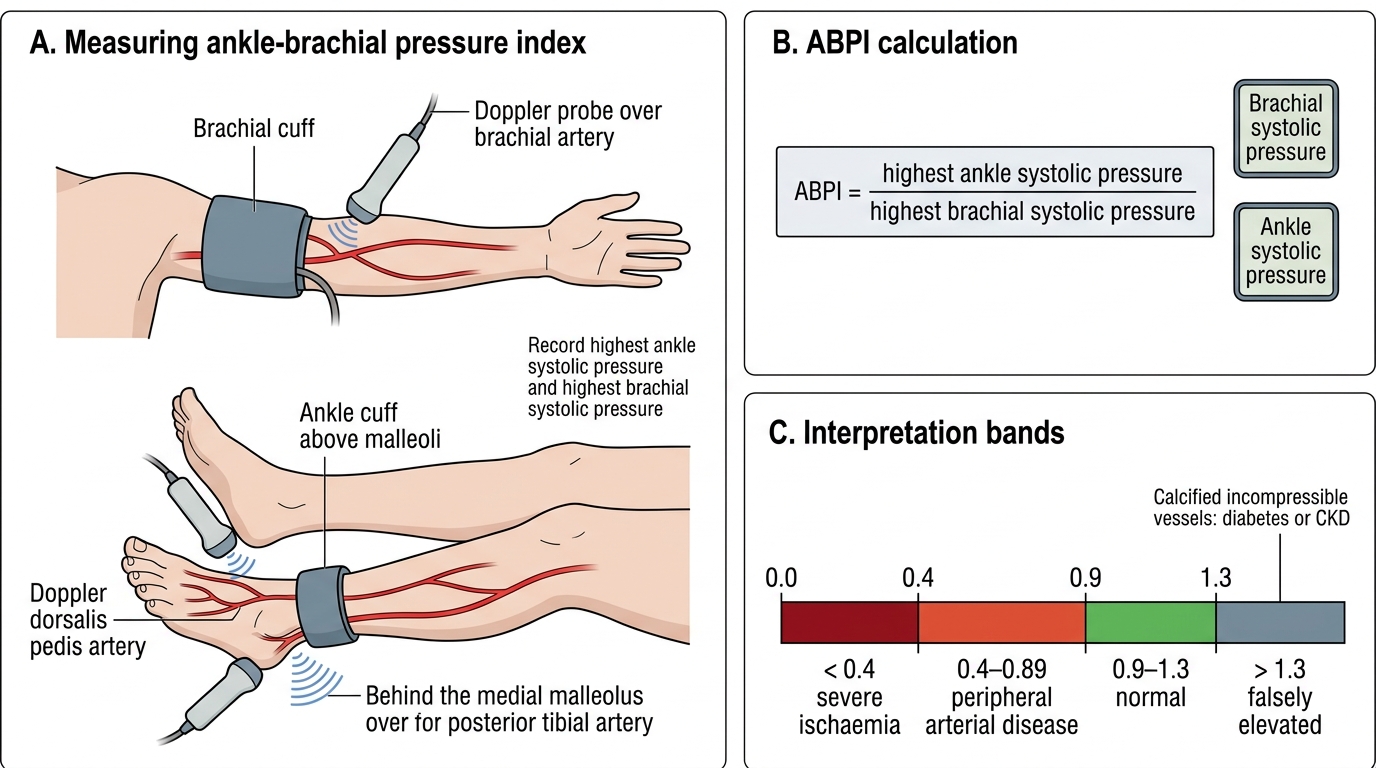
The peripheral arterial examination is a set-piece that should be performed and recorded the same way every time, and most of the diagnosis is made here. Inspect both legs for colour (pallor, dusky cyanosis), trophic changes (shiny hairless skin, brittle nails, muscle wasting), and tissue loss — ulcers (arterial ulcers are typically painful, punched-out and over pressure points or the toes) and gangrene. Palpate temperature and capillary refill, then systematically feel the femoral, popliteal, posterior tibial and dorsalis pedis pulses, comparing sides, and auscultate for femoral bruits. Perform Buerger's test: elevate the leg and watch for pallor (a positive test, with the angle at which the limb blanches indicating severity), then sit the patient up with legs dependent and watch for the sluggish reactive hyperaemia (a dusky red 'sunset foot'). The single most useful bedside measurement is the ankle-brachial pressure index (ABPI) — the ratio of the highest ankle systolic pressure (by hand-held Doppler) to the higher brachial systolic pressure. Interpret it carefully: normal is 0.9–1.3; below 0.9 indicates peripheral arterial disease; below 0.4 indicates severe/critical ischaemia; and an index above 1.3 is falsely elevated, meaning non-compressible calcified vessels, classically in diabetes and chronic kidney disease — in those patients a normal or high ABPI does not exclude disease and you supplement with toe pressures or waveforms. Confirm and map the disease with imaging: arterial duplex ultrasound first (non-invasive, shows site and severity), then CT or MR angiography to plan intervention, with catheter (digital subtraction) angiography reserved for when endovascular treatment is being delivered at the same sitting.
Ankle-Brachial Pressure Index Measurement and Interpretation
- Inspect: colour, trophic changes, ulcers (painful, punched-out), gangrene.
- Palpate: temperature, capillary refill, femoral/popliteal/posterior tibial/dorsalis pedis pulses; femoral bruit.
- Buerger's test: elevation pallor angle + dependent reactive hyperaemia.
- ABPI: normal 0.9–1.3; <0.9 disease; <0.4 critical; >1.3 falsely high (calcified vessels — diabetes/CKD).
- Imaging: duplex → CT/MR angiography → catheter angiography (when treating).