Page 2 of 20
SU27.1-2 | Occlusive Arterial Disease — SDL Guide (Part 2)
Principles of Surgical and Medical Management
Management follows directly from where the patient sits on the spectrum, and it always begins with the systemic disease. For claudication, the foundation is best medical therapy and risk-factor modification: complete smoking cessation, a supervised exercise programme (which reliably improves walking distance by promoting collaterals), control of diabetes and hypertension, a statin and an antiplatelet agent (such as aspirin or clopidogrel) to reduce cardiovascular events. Most claudicants are managed this way and never need an operation; intervention is reserved for lifestyle-limiting symptoms that fail medical therapy. Critical limb-threatening ischaemia (rest pain, ulceration or gangrene) is different — the limb is at risk, so revascularisation is needed wherever feasible, by endovascular means (angioplasty with or without a stent, best for shorter, more proximal lesions) or surgical bypass (using vein or a prosthetic graft to carry blood around the blockage, better for long occlusions and good distal targets), alongside wound care and treatment of infection. Acute limb ischaemia is the emergency: recognise the six P's, give immediate intravenous heparin to limit propagation of clot, obtain urgent imaging if it will not delay treatment in a threatened limb, and restore flow by surgical embolectomy (a balloon catheter, classically for an embolus in a healthy vessel), catheter-directed thrombolysis or bypass depending on the cause and limb viability — with fasciotomy considered after reperfusion to prevent compartment syndrome. When the limb is unsalvageable — irreversible ischaemia with fixed mottling, muscle rigidity and paralysis, or spreading wet gangrene threatening life — amputation at the lowest viable level that will heal is the correct, life-preserving decision rather than a failure.
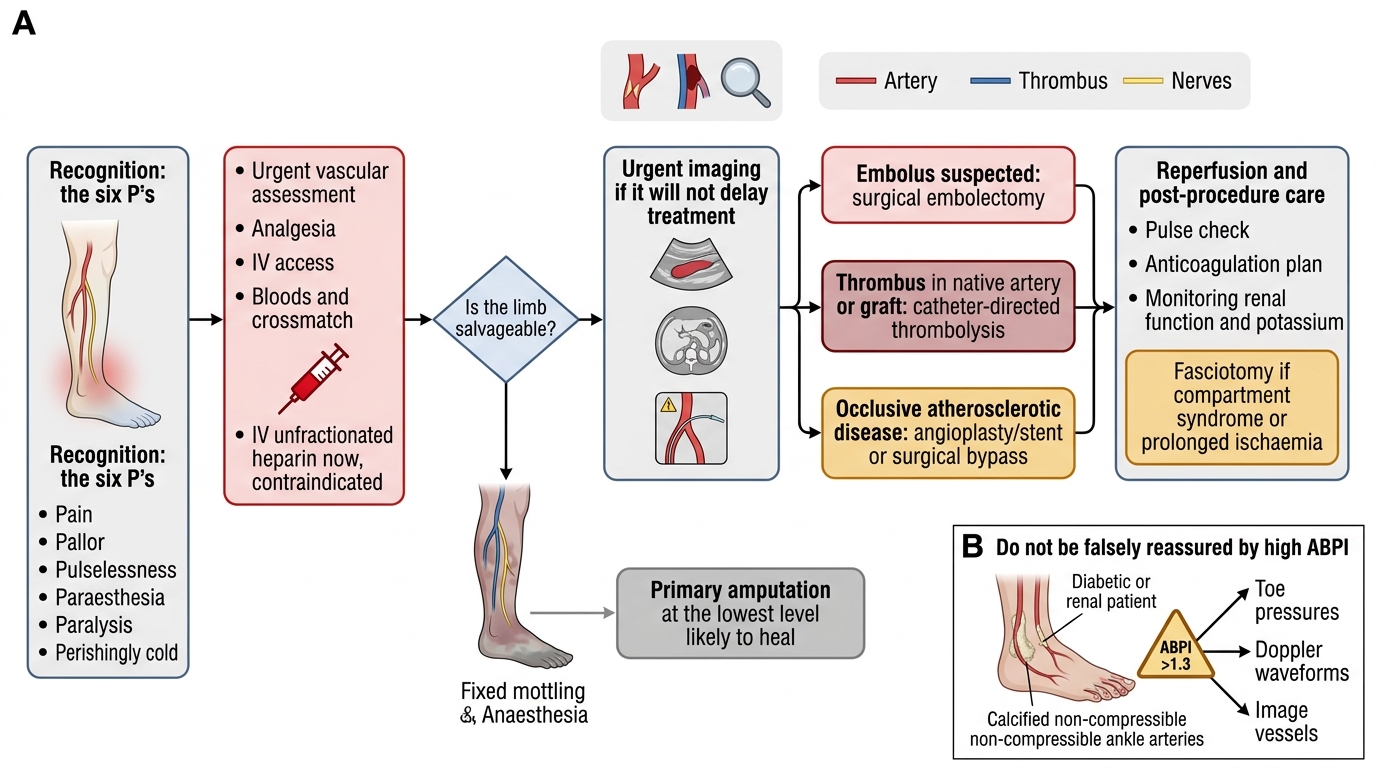
Management of Acute Limb Ischaemia
- Claudication: smoking cessation, supervised exercise, statin + antiplatelet, risk-factor control; intervene only if medical therapy fails.
- Critical limb ischaemia: revascularise — endovascular (angioplasty/stent) or surgical bypass — plus wound/infection care.
- Acute limb ischaemia: IV heparin now → embolectomy / thrombolysis / bypass; fasciotomy after reperfusion.
- Unsalvageable limb: amputation at the lowest level that will heal.
CLINICAL PEARL
Beware the falsely reassuring ABPI in a diabetic or renal patient. Medial arterial calcification makes the vessels non-compressible, so the ankle pressure — and therefore the ABPI — reads NORMAL or HIGH (>1.3) even when the foot is critically ischaemic. Never let an ABPI above 1.3 talk you out of a diagnosis the foot is shouting at you: if the toes are dusky, the ulcer will not heal, or rest pain is present, measure toe pressures or analyse Doppler waveforms and image the vessels. A high ABPI is a red flag, not the all-clear.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 62-year-old smoker with reproducible calf claudication that is now shortening, plus nocturnal forefoot rest pain relieved by dependency, has progressed along the chronic atherosclerotic spectrum towards critical limb ischaemia: he needs aggressive best medical therapy (smoking cessation, supervised exercise, statin, antiplatelet, glycaemic and blood-pressure control), an ABPI and duplex, and — because rest pain signals a threatened limb — assessment for revascularisation. The 70-year-old in atrial fibrillation with a sudden, white, numb, pulseless, cold leg has acute embolic limb ischaemia: she needs the six P's recognised at once, immediate intravenous heparin, and urgent embolectomy or thrombolysis before the muscle and nerve die — every hour counts. Use these to self-test the competencies this module covers. First, can you describe the etiopathogenesis of occlusive arterial disease — atherosclerosis versus Buerger's — and the claudication → rest pain → tissue loss spectrum with its Fontaine stages? Second, can you perform the peripheral arterial examination and measure and interpret an ABPI, including the falsely high reading in calcified diabetic vessels? Third, can you state the principles of treatment, distinguishing best medical therapy for claudication from urgent revascularisation for critical and acute ischaemia, and when amputation is the right choice? The questions that follow check exactly these links.
SELF-CHECK
A patient presents with a suddenly painful, pale, pulseless and cold leg that began 4 hours ago. Before any imaging, what is the most appropriate immediate medical step?
A. Start an oral antiplatelet and review in clinic
B. Give intravenous heparin to limit clot propagation
C. Elevate the limb to reduce swelling
D. Begin a supervised exercise programme
Reveal Answer
Answer: B. Give intravenous heparin to limit clot propagation
This is acute limb ischaemia (the six P's). Immediate intravenous heparin (anticoagulation) is given at once to limit propagation of thrombus while urgent imaging and definitive revascularisation (embolectomy, thrombolysis or bypass) are arranged. Elevation worsens perfusion, an oral antiplatelet with clinic review is far too slow for a threatened limb, and exercise programmes are for stable claudication, not an acutely ischaemic limb.