Page 4 of 20
SU27.3 | Vasospastic Disorders — SDL Guide
Learning Objectives
- Describe the clinical features of vasospastic disorders, principally Raynaud's phenomenon, and the colour sequence of an attack (SU27.3).
- Distinguish primary Raynaud's disease from secondary Raynaud's syndrome and outline the investigations and principles of management (SU27.3).
INSTRUCTIONS
Some arteries are not blocked but go into spasm — clamping down on exposure to cold or stress and then opening up again. Vasospastic disorders, of which Raynaud's phenomenon is the classic example, cause fingers and toes to change colour through a recognisable white-blue-red sequence. The clinically important task is to decide whether this is a benign, idiopathic condition (primary Raynaud's disease, common in young women) or the first sign of a serious underlying illness such as scleroderma (secondary Raynaud's syndrome). This module connects the physiology of reversible arterial spasm to the bedside discrimination of primary from secondary disease, the focused investigations that uncover an underlying cause, and the stepwise management from cold avoidance to drugs and, rarely, sympathectomy.
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old typist describes how, every winter, her fingers suddenly turn dead white when she steps outside or opens the freezer; within minutes they go a dusky blue, and as they warm up indoors they flush an angry, tingling red before returning to normal. Both hands are affected, symmetrically, and between attacks her hands look entirely normal. In the same clinic sits a 52-year-old man whose fingertips have begun to do something similar — but his attacks started only recently, affect his right hand more than his left, and he now has a small painful ulcer on one fingertip and tight, shiny skin over the backs of his fingers. The same colour change, yet one story is reassuring and the other is a warning. Learning to tell episodic, reversible arterial spasm from the spasm that heralds a dangerous underlying disease is the heart of this topic.
WHY THIS MATTERS
Vasospastic disorders are common and mostly benign, but they matter for two reasons. First, Raynaud's phenomenon is frequently the earliest manifestation of a serious connective-tissue disease — particularly systemic sclerosis (scleroderma) — sometimes appearing years before the diagnosis is otherwise made, so recognising the 'red flags' for secondary disease lets you investigate and refer early. Second, severe vasospasm can progress to genuine digital ischaemia, ulceration and even gangrene of the fingertips, which is painful, disabling and difficult to treat. As a clinician you will be asked to reassure the large majority with benign primary disease, while picking out the minority who need autoantibody testing and a rheumatology opinion. For a final-year student, distinguishing functional spasm from fixed occlusive arterial disease, and primary from secondary Raynaud's, is a classic clinical-reasoning exercise that is regularly examined.
RECALL
Recall the physiology this rests on. From PY: the tone of small arteries and arterioles is set by the smooth muscle in their walls, which constricts under sympathetic (alpha-adrenergic) drive and local mediators and relaxes when those fall — normal thermoregulation already shunts blood away from the skin in the cold. A vasospastic disorder is an exaggeration of this normal reflex: a reversible, excessive constriction of the digital arteries rather than a fixed structural blockage. Hold on to the contrast you learned in occlusive arterial disease — there, the artery is permanently narrowed or thrombosed and the limb is ischaemic continuously; here, the vessel is structurally normal (in primary disease) and the ischaemia comes and goes. This functional-versus-structural distinction is the key to understanding why the colour change is episodic and why the mainstay of treatment is to relax the vessel and avoid the trigger.
Fingers that Turn White in the Cold
The hallmark of Raynaud's phenomenon is an episodic, well-demarcated colour change in the digits provoked by cold or emotional stress, and the classic attack runs through a triphasic colour sequence: white → blue → red. The fingers (and sometimes toes, nose or ears) first go white (pallor) as the digital arteries spasm and shut off blood flow, giving cold, numb, sharply demarcated digits; they then turn blue (cyanosis) as the stagnant blood in the capillaries gives up its oxygen; and finally, on rewarming, they flush red (rubor) as the spasm relaxes and reactive hyperaemia floods the tissue, often with throbbing, tingling and pain. Between attacks the hands typically look normal. The history is what first separates benign from worrying disease. Primary Raynaud's disease typically begins in young women (often under 30), is bilateral and symmetrical, is triggered reproducibly by cold and stress, and crucially causes no tissue loss and no underlying illness. By contrast, features that point to a secondary cause and demand investigation are: onset at an older age, asymmetry between the hands, digital ulcers, scarring or gangrene, severe or progressive attacks, and accompanying symptoms of a connective-tissue disease (tight skin, arthralgia, dysphagia, dry eyes and mouth). Asking carefully about occupation (vibrating tools), drugs (beta-blockers, ergot derivatives) and these systemic features steers the whole work-up before you have examined the hands.
The Vascular Basis of Vasospasm and its Classification
Vasospastic disorders are conditions of reversible, exaggerated arterial spasm rather than fixed structural occlusion, and Raynaud's phenomenon is classified by whether or not there is an underlying cause. Primary Raynaud's (Raynaud's disease) is idiopathic — an isolated abnormality of vasomotor control with no associated illness; it is common, affects young women, is symmetrical, and does not cause tissue loss; the digital vessels are structurally normal and the prognosis is benign. Secondary Raynaud's (Raynaud's syndrome/phenomenon) is vasospasm occurring as part of, or because of, another disease, and here structural vessel damage may coexist so that digital ulceration and gangrene can occur. The important causes to know are: connective-tissue diseases — above all systemic sclerosis (scleroderma), but also SLE, mixed connective-tissue disease and dermatomyositis; occupational vibration injury (hand-arm vibration syndrome from chainsaws, drills); thoracic outlet / cervical rib compressing the subclavian artery; drugs (beta-blockers, ergot alkaloids); and underlying atherosclerotic or embolic arterial disease. Two related vasomotor conditions are worth recognising and not confusing with Raynaud's: acrocyanosis (persistent, painless blue discolouration of the hands without the triphasic sequence) and chilblains (pernio) (itchy, inflamed cold-induced skin lesions). The central clinical task is therefore to classify any Raynaud's as primary or secondary, because the classification dictates both the investigation and the seriousness.
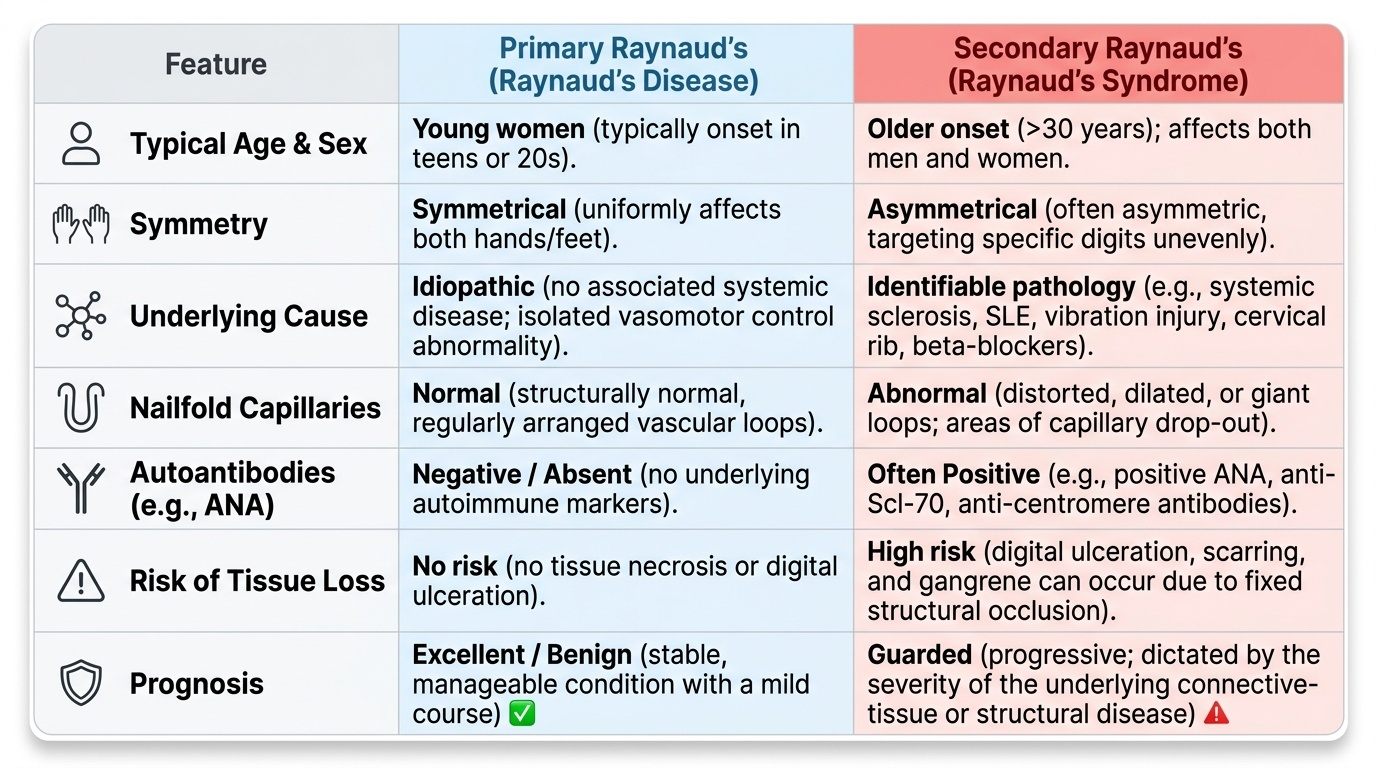
Provided image
- Primary (Raynaud's disease): idiopathic, young women, symmetrical, no tissue loss, normal vessels, benign.
- Secondary (Raynaud's syndrome): an identifiable cause; may have ulcers/gangrene and abnormal investigations.
- Causes of secondary disease: connective-tissue disease (esp. scleroderma), vibration injury, thoracic outlet/cervical rib, drugs, atherosclerotic/embolic disease.
- Related entities: acrocyanosis (persistent painless cyanosis), chilblains (pernio).
SELF-CHECK
During a typical Raynaud's attack, what is the correct sequence of colour change in the fingers?
A. Red → white → blue
B. Blue → red → white
C. White (pallor) → blue (cyanosis) → red (reactive hyperaemia)
D. White → red → blue
Reveal Answer
Answer: C. White (pallor) → blue (cyanosis) → red (reactive hyperaemia)
The classic triphasic Raynaud sequence is white → blue → red: pallor first as the digital arteries spasm and cut off flow, then cyanosis as stagnant capillary blood desaturates, then rubor (reactive hyperaemia) on rewarming as the spasm relaxes and blood floods back, often with tingling and pain.
Examination and Investigation
Examination is directed at confirming vasospasm and, above all, at hunting for an underlying cause that would make this secondary disease. Inspect the digits for colour (they are often normal between attacks), for trophic or ischaemic changes — digital pitting scars, ulcers or gangrene of the fingertips (which strongly suggest secondary disease), and for skin tightening or telangiectasia of scleroderma. Palpate all the peripheral pulses (brachial, radial, ulnar and the lower-limb pulses), because absent pulses point to fixed occlusive arterial disease rather than pure spasm, and examine the neck and arm for signs of a cervical rib or thoracic outlet syndrome. Examine the nailfold capillaries (with a dermatoscope or ophthalmoscope): dilated, dropped-out or distorted capillaries are a hallmark of an underlying connective-tissue disease, whereas normal nailfold capillaries support primary disease. Investigation is then targeted: a full blood count, ESR and autoantibody screen — antinuclear antibody (ANA) and, if positive, specific antibodies such as anti-centromere and anti-Scl-70 — to detect connective-tissue disease; cold-provocation or thermography may document the vasospasm objectively; and where fixed arterial disease or thoracic outlet compression is suspected, duplex ultrasound or angiography and a cervical-spine radiograph for a cervical rib. In short, normal pulses, normal nailfolds and negative autoantibodies in a young woman support a benign primary diagnosis, whereas abnormalities in any of these mandate a search for the underlying disease.
- Inspect: digital colour, pitting scars/ulcers/gangrene (→ secondary), scleroderma skin changes.
- Palpate: all peripheral pulses (absent → fixed occlusive disease); examine for cervical rib/thoracic outlet.
- Nailfold capillaroscopy: abnormal capillaries → connective-tissue disease.
- Bloods: FBC, ESR, ANA and specific autoantibodies (anti-centromere, anti-Scl-70).
- Imaging: duplex/angiography and cervical-spine X-ray when fixed disease or thoracic outlet is suspected.