Page 5 of 20
SU27.3 | Vasospastic Disorders — SDL Guide (Part 2)
Principles of Management
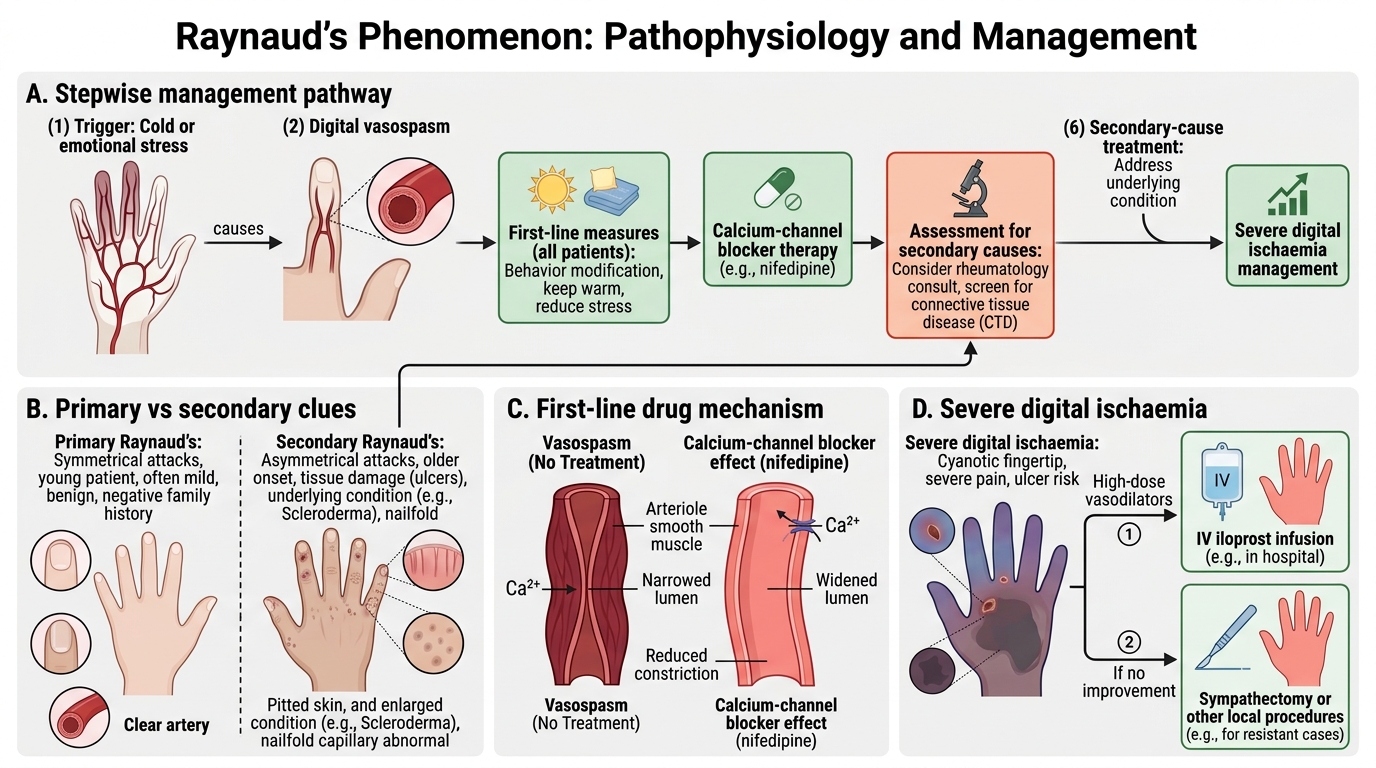
Management is stepwise and begins, in every case, with conservative measures and treating any underlying cause. The first line for all patients is avoidance of triggers: keeping the whole body and the hands warm (gloves, hand-warmers), avoiding sudden cold exposure, stopping smoking (which causes vasoconstriction and worsens attacks), and withdrawing precipitating drugs such as beta-blockers and ergot derivatives. Where Raynaud's is secondary, treating the underlying connective-tissue disease, removing vibration exposure, or relieving a cervical rib/thoracic outlet is essential. When attacks remain frequent or severe despite conservative measures, the first-line pharmacological treatment is a calcium-channel blocker (such as nifedipine), which relaxes vascular smooth muscle and reduces the frequency and severity of attacks; other vasodilators may be added. For severe digital ischaemia with ulceration or threatened gangrene, more aggressive options are used: intravenous prostacyclin (iloprost) infusions to promote vasodilatation and healing, and, in resistant cases, sympathectomy (chemical or surgical interruption of the sympathetic supply to abolish vasoconstrictor tone) or local digital procedures — though sympathectomy gives less durable benefit in the upper limb. The overall principle is to escalate from trigger avoidance and underlying-disease control, through vasodilator drugs, to interventional measures only for limb- or digit-threatening ischaemia.
Stepwise Management of Raynaud's Phenomenon
- First line (all patients): keep warm, avoid cold, stop smoking, withdraw precipitating drugs; treat the underlying cause if secondary.
- Drug of first choice: calcium-channel blocker (nifedipine) for frequent/severe attacks.
- Severe digital ischaemia: IV prostacyclin (iloprost); sympathectomy or local procedures for resistant cases.
CLINICAL PEARL
Treat Raynaud's phenomenon as a clue, not just a complaint. The single most important decision is primary versus secondary — and the features that should make you suspect a serious underlying disease (and order an ANA and rheumatology referral) are: onset after about 30 years of age, asymmetry between the hands, digital ulcers or pitting scars, abnormal nailfold capillaries, and any accompanying connective-tissue symptoms such as tight skin, arthralgia or dysphagia. A young woman with symmetrical attacks, normal hands between episodes, normal pulses and a negative autoantibody screen has benign primary disease and can be reassured; a middle-aged patient with a fingertip ulcer cannot.
Check Your Understanding
Bring the threads together by reasoning back through the two patients in the hook. The 24-year-old typist with symmetrical, bilateral attacks, a classic white-blue-red sequence, normal hands between episodes and no tissue loss has primary Raynaud's disease: with normal pulses, normal nailfold capillaries and a negative autoantibody screen she can be reassured, advised on keeping warm and stopping any precipitating drugs, and given a calcium-channel blocker only if attacks are troublesome. The 52-year-old man with recent-onset, asymmetrical attacks, a painful fingertip ulcer and tight shiny skin has secondary Raynaud's syndrome, very likely heralding systemic sclerosis: he needs nailfold capillaroscopy, an ANA and specific autoantibodies, a rheumatology referral, aggressive warming and smoking cessation, a calcium-channel blocker, and — for the ischaemic ulcer — consideration of intravenous prostacyclin. Use these to self-test the competency this module covers. First, can you describe the clinical features of a vasospastic attack, including the triphasic colour sequence and its triggers? Second, can you distinguish primary from secondary Raynaud's by the red-flag features and the targeted investigations (pulses, nailfold capillaries, autoantibodies, imaging)? Third, can you state the stepwise principles of management from trigger avoidance and treating the underlying cause, through calcium-channel blockers, to prostacyclin or sympathectomy for severe digital ischaemia? The questions below check exactly these links.
SELF-CHECK
A 50-year-old man presents with recent-onset, asymmetrical Raynaud's attacks and a painful ulcer on one fingertip. Which feature most strongly indicates SECONDARY (rather than primary) Raynaud's, and what is the most appropriate next investigation?
A. His symmetrical attacks; measure ABPI
B. The digital ulcer and asymmetry; send an antinuclear antibody (ANA) screen
C. His young age; reassure and discharge
D. The triphasic colour change; no investigation needed
Reveal Answer
Answer: B. The digital ulcer and asymmetry; send an antinuclear antibody (ANA) screen
Digital ulceration, asymmetry and onset later in life are red flags for secondary Raynaud's, most often due to a connective-tissue disease such as systemic sclerosis. The appropriate next step is an autoantibody screen (ANA, then specific antibodies such as anti-centromere and anti-Scl-70), nailfold capillaroscopy and rheumatology referral. Primary Raynaud's, by contrast, is symmetrical, occurs in young women and causes no tissue loss.