Page 11 of 17
SU28.18 | Clinical Examination of Abdomen — SDL Guide (Part 2)
Eliciting and Interpreting Key Signs
Beyond the routine, a handful of special signs answer specific questions, and you must know how to elicit and interpret each. To detect free fluid (ascites), use shifting dullness: percuss from the resonant centre outwards to the dull flank, mark the level, then roll the patient towards you and re-percuss — if the dullness has 'shifted' (the previously dull flank becomes resonant as fluid moves), ascites is present (demonstrable with roughly 500 mL or more). For larger, tense ascites, elicit a fluid thrill: with an assistant's hand on the midline to damp the fat wave, flick one flank and feel the transmitted wave at the other. To assess organomegaly, distinguish an enlarged spleen (enlarges towards the right iliac fossa, moves down on inspiration, has a notch, is dull to percussion, and you cannot get above it) from an enlarged left kidney (lies in the loin, is ballotable bimanually, moves only slightly with respiration, and has a band of colonic resonance in front of it). To characterise a mass, determine whether it is parietal (in the abdominal wall — it becomes more prominent and remains palpable when the patient tenses the abdominal muscles by lifting the head or legs: a positive Carnett's/rising test) or intra-abdominal (it becomes less palpable when the muscles are tensed), and whether an intra-abdominal mass is mobile (intraperitoneal) or fixed and non-moving with respiration (retroperitoneal). Finally, the signs of peritonism — guarding, rigidity and rebound tenderness — indicate parietal peritoneal irritation and an acute abdomen. Interpreting these signs correctly is what converts a list of findings into a diagnosis.
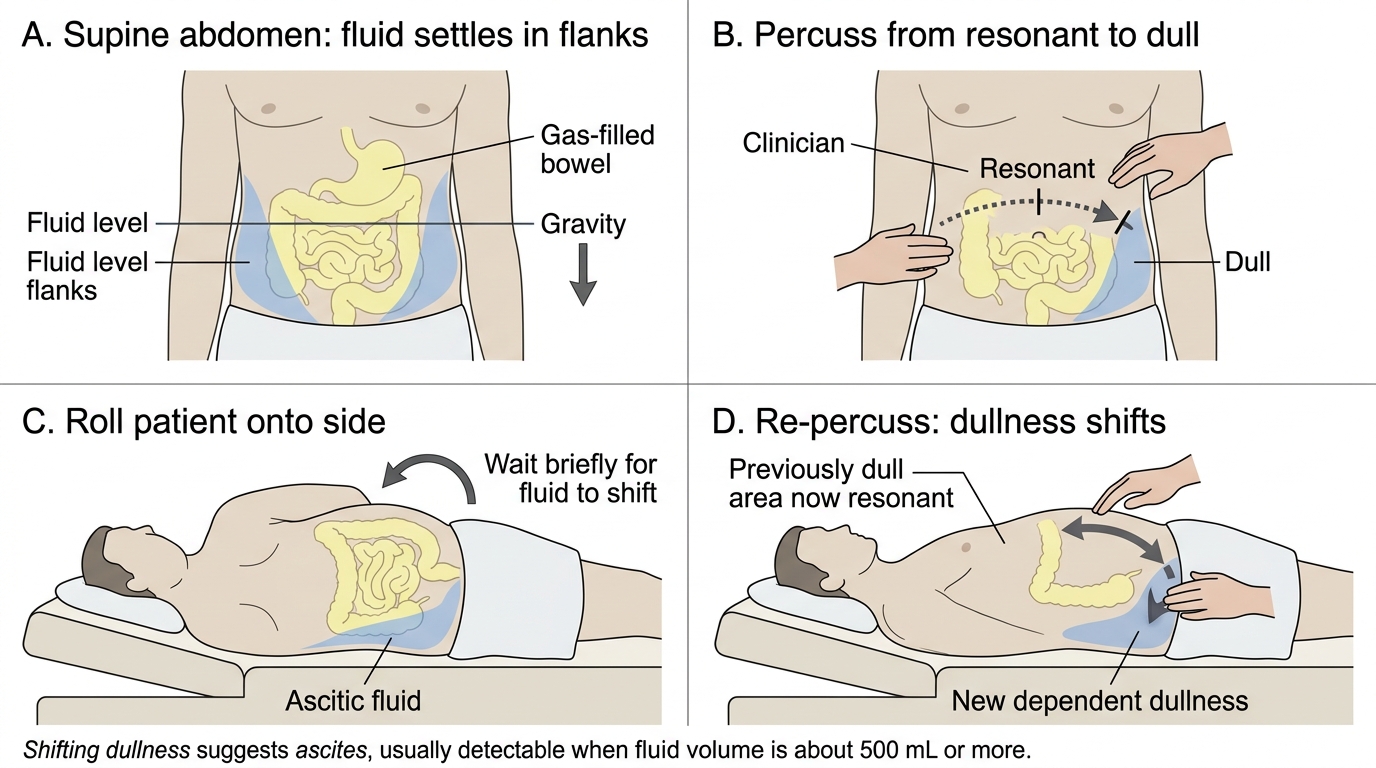
Eliciting Shifting Dullness in Ascites
- Ascites: shifting dullness (>=~500 mL); fluid thrill (large tense ascites).
- Splenomegaly: towards RIF, moves with respiration, notch, dull, cannot get above it.
- Renal mass: ballotable, in the loin, band of resonance in front, little respiratory movement.
- Mass: parietal (more prominent on tensing — positive rising test) vs intra-abdominal (less palpable on tensing); mobile vs fixed (retroperitoneal).
- Peritonism: guarding, rigidity, rebound.
CLINICAL PEARL
Use two quick tests to classify any abdominal lump. First, the 'getting above it' and notch test separates a big spleen from a big kidney: you cannot get above an enlarged spleen, it has a notch and is dull, whereas a renal mass is ballotable with a band of resonance in front. Second, the rising (Carnett's) test separates a wall lump from a deep one: ask the patient to lift their head or straight legs to tense the abdominal muscles — a parietal (wall) mass becomes MORE prominent and stays palpable, while a true intra-abdominal mass becomes LESS palpable as the tensed muscles guard it. These two bedside manoeuvres save many unnecessary scans.
From Findings to Investigations and a Treatment Plan
The examination is only useful if it drives the next steps, so the final skill is turning findings into an appropriate, problem-oriented work-up and plan. Let the findings choose the investigations: a rigid, peritonitic abdomen prompts urgent bloods (full blood count, urea and electrolytes, amylase/lipase), an erect chest X-ray for free gas under the diaphragm and often a contrast-enhanced CT; organomegaly or a mass prompts bloods appropriate to the suspected cause and an ultrasound (often followed by CT to characterise and stage); ascites prompts ultrasound and a diagnostic ascitic tap (cell count, protein, cytology, culture); obstruction prompts an abdominal X-ray and CT; and suspected luminal pathology prompts endoscopy. Investigations should be targeted by the clinical question, not ordered as an indiscriminate panel. From the synthesis of history, examination and results, construct a problem-oriented treatment plan: state the working diagnosis and differential, the immediate management (for example resuscitation and analgesia in an acute abdomen, or referral for drainage of a collection), the definitive treatment options (conservative, medical or surgical) and the follow-up. Equally important is to document the findings clearly — the regions examined, the signs elicited and not elicited — so that another clinician can follow your reasoning and detect change over time. This closes the loop the competency requires: examine, order relevant investigations, and discuss an appropriate treatment plan.
Provided image
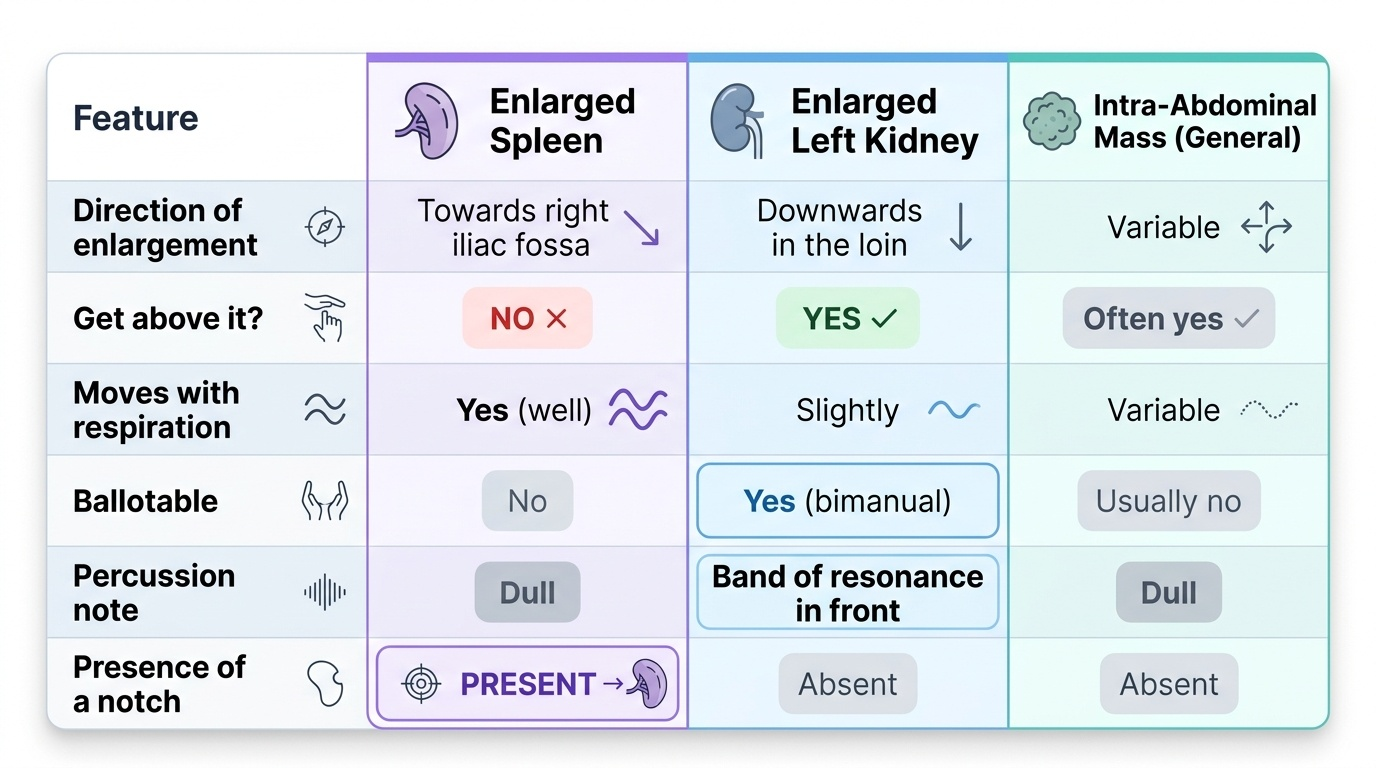
| Feature | Enlarged spleen | Enlarged left kidney | Intra-abdominal mass (general) |
|---|---|---|---|
| Direction of enlargement | Towards right iliac fossa | Downwards in the loin | Variable |
| Get above it? | No | Yes | Often yes |
| Moves with respiration | Yes (well) | Slightly | Variable |
| Ballotable | No | Yes (bimanual) | Usually no |
| Percussion | Dull | Band of resonance in front | Dull |
| Notch | Present | Absent | Absent |
Check Your Understanding
Bring the whole skill together by walking through the patient in the hook. The registrar prepared the patient (exposure, right side, asked about pain), inspected the contour and movement, palpated light then deep and felt a left-upper-quadrant mass, percussed a dull band over it, auscultated, and then used special signs — she could not get above the mass, it moved down on inspiration and had a notch (splenomegaly, distinguished from a renal mass), and the flanks showed shifting dullness (ascites) — and finally translated these findings into an appropriate plan: targeted bloods, an ultrasound and an ascitic tap. Use this to self-test the competency on four links. First, can you state the four-step sequence — inspect, palpate, percuss, auscultate — and the preparation that makes it reliable (consent, exposure, warm hands, right side, ask about pain and start away from it, complete with hernial orifices and per-rectal)? Second, can you elicit and interpret the key signs — shifting dullness and fluid thrill for ascites, the spleen-versus-kidney distinction, the parietal-versus-intra-abdominal mass test, and peritonism? Third, can you let the findings drive relevant, targeted investigations rather than a blind panel? Fourth, can you construct and document a problem-oriented treatment plan? The questions below check exactly these.
SELF-CHECK
On examining a left upper quadrant swelling you find that you cannot get above it, it moves down with inspiration, it has a palpable notch, and it is dull to percussion. Which is the most likely structure?
A. An enlarged left kidney
B. An enlarged spleen
C. A retroperitoneal tumour
D. A faecal-loaded descending colon
Reveal Answer
Answer: B. An enlarged spleen
Inability to get above the swelling, good downward movement with respiration, a palpable notch and dullness to percussion are the classic features of an enlarged SPLEEN. An enlarged kidney is ballotable, lies in the loin, moves only slightly with respiration and has a band of colonic resonance in front of it; a retroperitoneal mass is fixed and does not move with respiration.