Page 4 of 20
SU28.14 | Disorders of Small Intestine and Large Intestine — SDL Guide
Learning Objectives
- Describe the clinical features of the major disorders of the small and large intestine — obstruction, intussusception, volvulus, inflammatory bowel disease and colorectal carcinoma — including neonatal obstruction and short-gut syndrome (SU28.14).
- Outline the appropriate investigations for these disorders, including the plain abdominal radiograph, contrast/CT studies, colonoscopy with biopsy and tumour markers (SU28.14).
- Describe the principles of medical and surgical management of intestinal disorders (SU28.14).
INSTRUCTIONS
The small and large intestine fail in a small number of recognisable ways — they obstruct, they bleed, they inflame, and they grow cancers — and almost every emergency and elective bowel operation answers one of these. This module builds directly on the intestinal anatomy you have learned: the SMA/IMA blood supply, the watershed zones, and the valvulae-versus-haustra distinction on the X-ray all reappear here as the basis for diagnosis and surgery. The clinical pay-off is the ability to separate small-bowel from large-bowel obstruction, recognise the surgical emergencies, and reason out an evidence-based work-up of altered bowel habit and rectal bleeding.
References
- Bailey & Love's Short Practice of Surgery, Intestinal Obstruction and The Colon, Rectum and Anus (textbook)
- SRB's Manual of Surgery, Intestinal Obstruction and Colorectal Carcinoma (textbook)
- Sabiston Textbook of Surgery, Small Intestine and Colon and Rectum (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients arrive on the same surgical take. The first, a 30-year-old who had an appendicectomy a decade ago, has colicky central abdominal pain, several bilious vomits and a softly distended abdomen. The second, a 68-year-old, has months of increasingly altered bowel habit, dark blood mixed in the stool and a few kilograms of unexplained weight loss, and now cannot pass flatus. The third, a previously well infant, draws up his legs in spasms of screaming, passes a stool like red-currant jelly, and has a sausage-shaped mass in the right abdomen. Three different ages, three different stories — yet all three are disorders of the same two organs, the small and large intestine, and your task is to recognise the pattern, choose the right investigation, and know when the answer is an operation. This module gives you that framework.
WHY THIS MATTERS
Disorders of the intestine are the bread and butter of general surgery and a major part of the acute take. Intestinal obstruction alone accounts for a large share of emergency laparotomies, colorectal cancer is one of the commonest solid tumours you will encounter, and missing a strangulating obstruction or a closed loop costs lives. Getting the basics right — distinguishing small-bowel from large-bowel obstruction on the film, recognising the red flags of colorectal cancer, knowing that a large-bowel obstruction in an adult is cancer until proven otherwise, and spotting the surgical emergencies of strangulation and volvulus — is exactly what is expected of a final-year student and a house officer. The competency also demands the special situations of neonatal obstruction and short-gut syndrome, which test whether you can apply the same reasoning to the extremes of bowel length and age.
RECALL
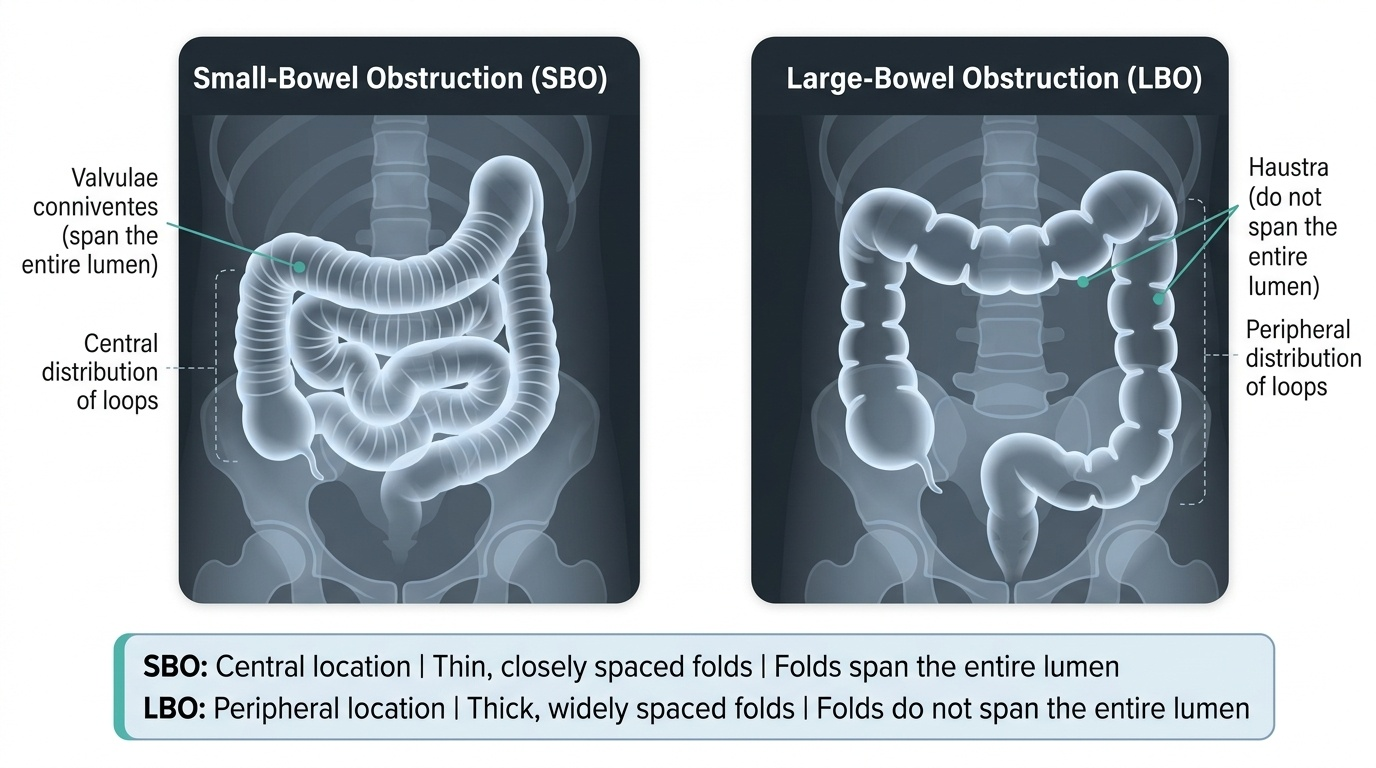
Recall the intestinal anatomy you have just studied, because every diagnosis here depends on it. The small bowel shows valvulae conniventes that cross the whole lumen and sits centrally on a plain film; the large bowel shows haustra that do not cross the lumen and frames the abdomen peripherally — this single distinction tells small-bowel from large-bowel obstruction. The bowel is supplied by the superior mesenteric artery (midgut) and inferior mesenteric artery (hindgut), so impairing that supply (a twist, a band, a strangulated hernia) makes the bowel ischaemic. Recall too that the ileocaecal valve, if competent, can convert a large-bowel obstruction into a dangerous closed loop, and that colonic veins drain to the portal system and the liver — the first site of colorectal metastasis. Hold these onto, and the disorders below become applied anatomy rather than a list.
The Patient with Obstruction, Bleeding or Altered Bowel Habit
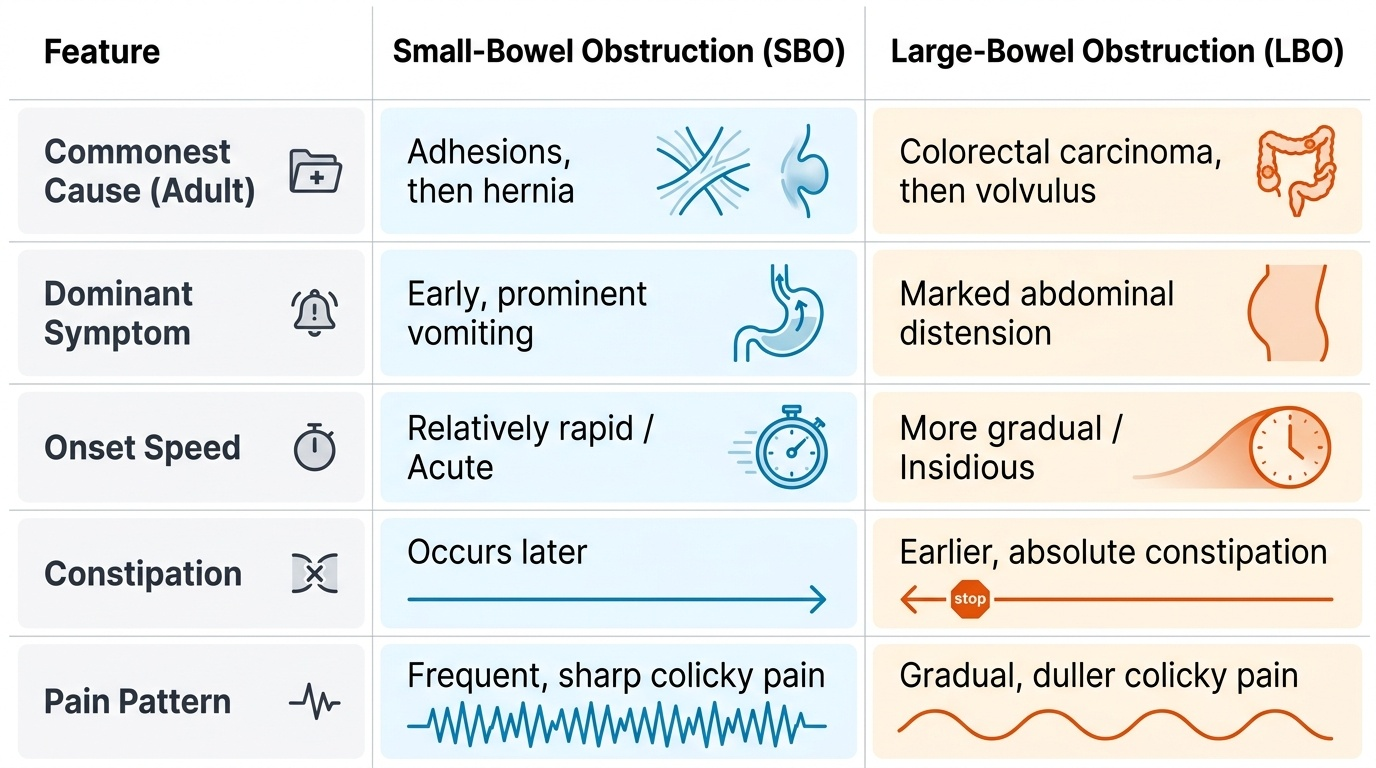
Intestinal disorders declare themselves through a small number of cardinal presentations, and learning to sort by these is more useful than memorising diseases. The first is intestinal obstruction, whose four classic features are colicky abdominal pain, vomiting, distension and absolute constipation (no faeces and no flatus); the balance of these features tells you the level. Small-bowel obstruction (SBO) presents early with prominent vomiting (bilious, then faeculent), central colicky pain and relatively little distension, and its commonest causes are post-operative adhesions and then hernia. Large-bowel obstruction (LBO) presents later with prominent distension, more gradual onset and earlier absolute constipation, and its commonest cause in an adult is colorectal carcinoma, then volvulus and diverticular stricture. The second presentation is rectal bleeding and altered bowel habit, the hallmark of colorectal cancer and inflammatory bowel disease. The third is the acute abdomen of strangulation — constant (not colicky) pain, tenderness, tachycardia and signs of peritonism — which marks compromised blood supply and demands urgent surgery. Recognising which pattern a patient fits is the first and most important diagnostic step.
Provided image
| Feature | Small-bowel obstruction | Large-bowel obstruction |
|---|---|---|
| Commonest cause (adult) | Adhesions, then hernia | Colorectal carcinoma, then volvulus |
| Dominant symptom | Early, prominent vomiting | Marked distension |
| Onset | Relatively rapid | More gradual |
| Constipation | Later | Earlier (absolute) |
Pathology and Surgical Basis of Intestinal Disorders
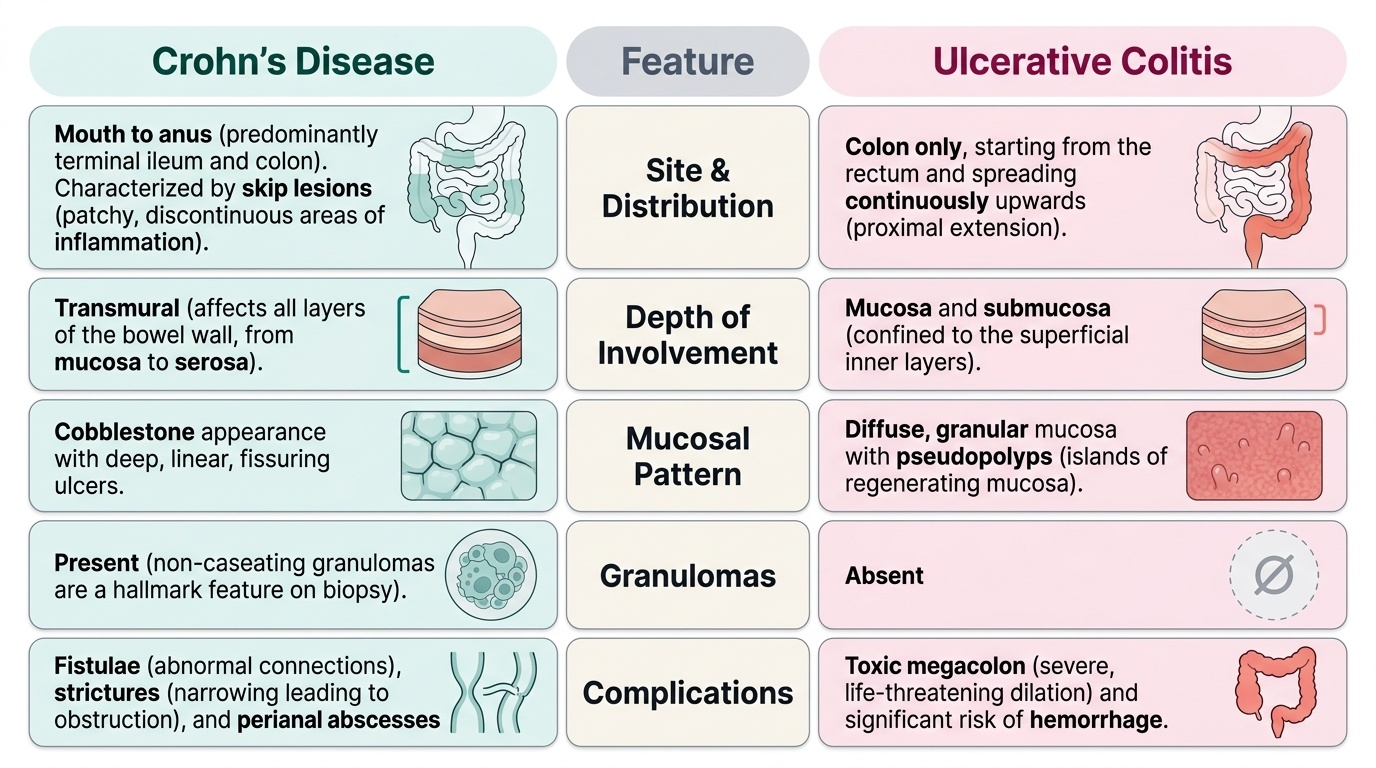
Behind these presentations lie a few mechanisms. Mechanical obstruction can be simple (lumen blocked, blood supply intact) or strangulating (blood supply compromised, bowel becomes ischaemic and will perforate) — the distinction is the whole game, because strangulation needs emergency surgery. A closed-loop obstruction, where bowel is blocked at two points (as in a volvulus or an LBO with a competent ileocaecal valve), is especially dangerous because pressure rises with nowhere to vent, threatening perforation (by Laplace's law the thin-walled, wide caecum perforates first). Two specific mechanisms deserve naming. Intussusception is the telescoping of one bowel segment into the next, classically ileocolic in infants (often after a viral illness causing lymphoid hyperplasia as the lead point), producing colicky pain, a sausage-shaped mass and red-currant-jelly stool, with a target/doughnut sign on ultrasound. Volvulus is a twist of bowel on its mesentery, most often the sigmoid colon in older or constipated patients, giving a massively distended loop and the coffee-bean (omega) sign on the film. Inflammatory bowel disease divides into Crohn's disease (transmural, skip lesions, mouth-to-anus, granulomas, prone to fistulae and strictures) and ulcerative colitis (mucosal, continuous, rectum-upwards, no granulomas, risk of toxic megacolon). Colorectal carcinoma develops through the adenoma–carcinoma sequence from a benign polyp, which is why screening and polypectomy work. Finally, the competency demands two extremes: neonatal obstruction (duodenal/jejunoileal atresia, malrotation with midgut volvulus, Hirschsprung's disease, meconium ileus, anorectal malformation) and short-gut syndrome (malabsorption after extensive small-bowel resection, typically when under ~200 cm remains).
Provided image
| Feature | Crohn's disease | Ulcerative colitis |
|---|---|---|
| Site | Mouth to anus (often terminal ileum) | Colon only, from rectum upwards |
| Depth | Transmural | Mucosa/submucosa |
| Distribution | Skip lesions | Continuous |
| Mucosa | Cobblestoning, deep fissuring ulcers | Diffuse, granular, pseudopolyps |
| Granulomas | Present (non-caseating) | Absent |
| Complications | Fistulae, strictures, abscess | Toxic megacolon, higher cancer risk |
SELF-CHECK
An infant presents with episodic colicky pain, a sausage-shaped abdominal mass and a red-currant-jelly stool. What is the diagnosis and the classic ultrasound sign?
A. Sigmoid volvulus; coffee-bean sign
B. Intussusception; target (doughnut) sign
C. Hirschsprung's disease; double-bubble sign
D. Pyloric stenosis; string sign
Reveal Answer
Answer: B. Intussusception; target (doughnut) sign
The triad of colicky pain, a sausage-shaped mass and red-currant-jelly stool in an infant is classic ileocolic intussusception, which shows a target/doughnut sign on ultrasound. The coffee-bean sign is sigmoid volvulus; the double-bubble is duodenal atresia; the string sign is pyloric stenosis.
Examination and Investigation
Examination is directed at confirming the pattern and detecting danger. In suspected obstruction, look for distension, listen for the high-pitched/'tinkling' or absent bowel sounds, examine every hernial orifice (a strangulated hernia is a readily missed, readily treatable cause), and perform a digital rectal examination (an empty rectum, a mass, or blood). Constant tenderness, guarding, tachycardia and fever signal strangulation or perforation. The plain abdominal radiograph remains the key first investigation in obstruction: central loops with valvulae conniventes that span the lumen indicate SBO, peripheral loops with haustra indicate LBO, and a massive 'coffee-bean' loop suggests sigmoid volvulus. A contrast-enhanced CT of the abdomen is now the investigation of choice in most adult obstruction — it shows the level, the cause, a transition point, and signs of ischaemia or closed loop. For suspected colorectal cancer or IBD, colonoscopy with biopsy is definitive (visualising and sampling the lesion); carcinoembryonic antigen (CEA) is a tumour marker used for follow-up rather than diagnosis; and staging uses CT chest/abdomen/pelvis with MRI rectum for rectal tumours. Routine bloods (FBC for anaemia, U&E for the dehydration of vomiting, CRP, group-and-save) complete the work-up. In neonatal obstruction the approach is tailored — an abdominal film (double-bubble in duodenal atresia), contrast studies, and a rectal biopsy for Hirschsprung's.
Provided image
- Plain AXR: central valvulae (SBO) vs peripheral haustra (LBO); coffee-bean = sigmoid volvulus.
- Contrast CT abdomen: level, cause, transition point, ischaemia/closed loop — investigation of choice in adult obstruction.
- Colonoscopy + biopsy: definitive for colorectal cancer and IBD; CEA for follow-up, not diagnosis.
- Staging: CT chest/abdomen/pelvis; MRI rectum for rectal cancer.