Page 10 of 26
SU29.11 | Urethral Strictures — SDL Guide
Learning Objectives
- Describe the clinical features of urethral stricture, recognising the pattern of obstructive voiding symptoms and its complications (SU29.11).
- Explain the anatomy of the male urethra and the aetiopathogenesis of stricture (spongiofibrosis), with trauma as the major cause (SU29.11).
- Outline the examination and the key investigations of a urethral stricture, with the retrograde urethrogram as the central imaging study (SU29.11).
- Describe the principles of management — dilatation, direct vision internal urethrotomy and urethroplasty — selected by stricture length and site (SU29.11).
INSTRUCTIONS
A man who has to strain to pass a thin, splayed stream is describing obstruction, and in the male urethra one of the commonest mechanical causes is a stricture — a scarred, narrowed segment that will not stretch. The clinical task is to recognise the obstructive picture, trace it to its cause (most often old trauma), confirm and map the narrowing with a retrograde urethrogram, and then match the treatment to the stricture: a short bulbar narrowing and a long dense one are not treated the same way. This module connects the surgical anatomy of the urethra to a disciplined work-up and to a length-driven choice between dilatation, internal urethrotomy and definitive urethroplasty.
References
- Bailey & Love's Short Practice of Surgery, The Urethra and Penis (textbook)
- SRB's Manual of Surgery, Urethra — Stricture Urethra (textbook)
- Sabiston Textbook of Surgery, Urology — Urethral Stricture Disease (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 30-year-old man comes to clinic embarrassed that, over the past year, his urinary stream has slowly become weak and split into a thin spray that sometimes wets his shoes. He now has to stand and strain for a while before flow begins, and when he finishes he still feels his bladder is not empty. Two years ago he fell astride a steel bar while climbing a wall and passed bloodstained urine for a day before it settled, and he thought no more of it. He has since had one episode of fever with painful retention that needed a catheter. The story he is telling — slow, progressive obstruction after a forgotten perineal injury — points away from the prostate that troubles older men and towards a scarred, narrowed urethra. Everything you examine, request and decide flows from understanding that scar.
WHY THIS MATTERS
Urethral stricture is a disease that quietly degrades a young man's quality of life and, if neglected, threatens his kidneys. The obstruction it causes is mechanical and fixed — it will not respond to the drugs that help prostatic obstruction — so recognising it and treating the narrowing itself is the only solution. It matters to you as a future clinician for three practical reasons. First, you must not mistake it for benign prostatic obstruction in the wrong age group, or you will prescribe useless tablets while back-pressure damages the upper tracts. Second, a large share of strictures are iatrogenic — caused by rough catheterisation and careless instrumentation — so gentle technique is something you yourself control. Third, the management decision is a clean teaching example of matching an operation to anatomy: a short stricture and a long stricture demand different operations, and getting that choice right is the difference between a durable cure and a revolving door of repeat procedures.
RECALL
Recall the anatomy of the male urethra before we build on it, because every part of this topic depends on it. The male urethra is divided into an anterior urethra and a posterior urethra. The anterior urethra runs within the corpus spongiosum and has two parts — the penile (pendulous) urethra and the bulbar urethra — and it is the bulbar segment that is the commonest site of stricture. The posterior urethra has the membranous urethra, which pierces the urogenital diaphragm and is the narrowest, least mobile part, and the prostatic urethra above it. Hold on to one fact in particular: because the anterior urethra is wrapped by the vascular corpus spongiosum, scarring of a stricture is not confined to the lining but extends into this spongy tissue — a process called spongiofibrosis — which is why a stricture behaves as a rigid, non-distensible segment rather than a simple mucosal fold.
The Patient with Obstructive Voiding
A urethral stricture presents with the symptoms of mechanical bladder outlet obstruction, and the history is usually one of slow, insidious worsening over months to years rather than a sudden event. The cardinal complaint is a change in the urinary stream: it becomes weak and of poor force, and very characteristically it splays or sprays because the scarred segment deforms the exit jet. The patient learns to strain to void, describes hesitancy before flow begins and a prolonged time to empty, and is left with a sense of incomplete emptying and terminal dribbling from the residual urine that the obstructed bladder cannot expel. As obstruction progresses the consequences mount. Stagnant residual urine predisposes to recurrent urinary tract infection and to stone formation; the back-pressure can cause acute or chronic retention; and infection tracking through the scarred wall can produce a periurethral abscess or, if it discharges, a urethral fistula — the so-called "watering-can perineum" of multiple sinuses in long-neglected disease. Untreated, the sustained high pressure is transmitted upward and can cause back-pressure changes in the upper urinary tract and renal impairment. The history should also seek the cause: ask specifically about past perineal or straddle trauma, a pelvic fracture, previous catheterisation, instrumentation or endoscopic surgery, and past urethral infection or discharge, because these point directly to the aetiology and to the likely site and length of the stricture.
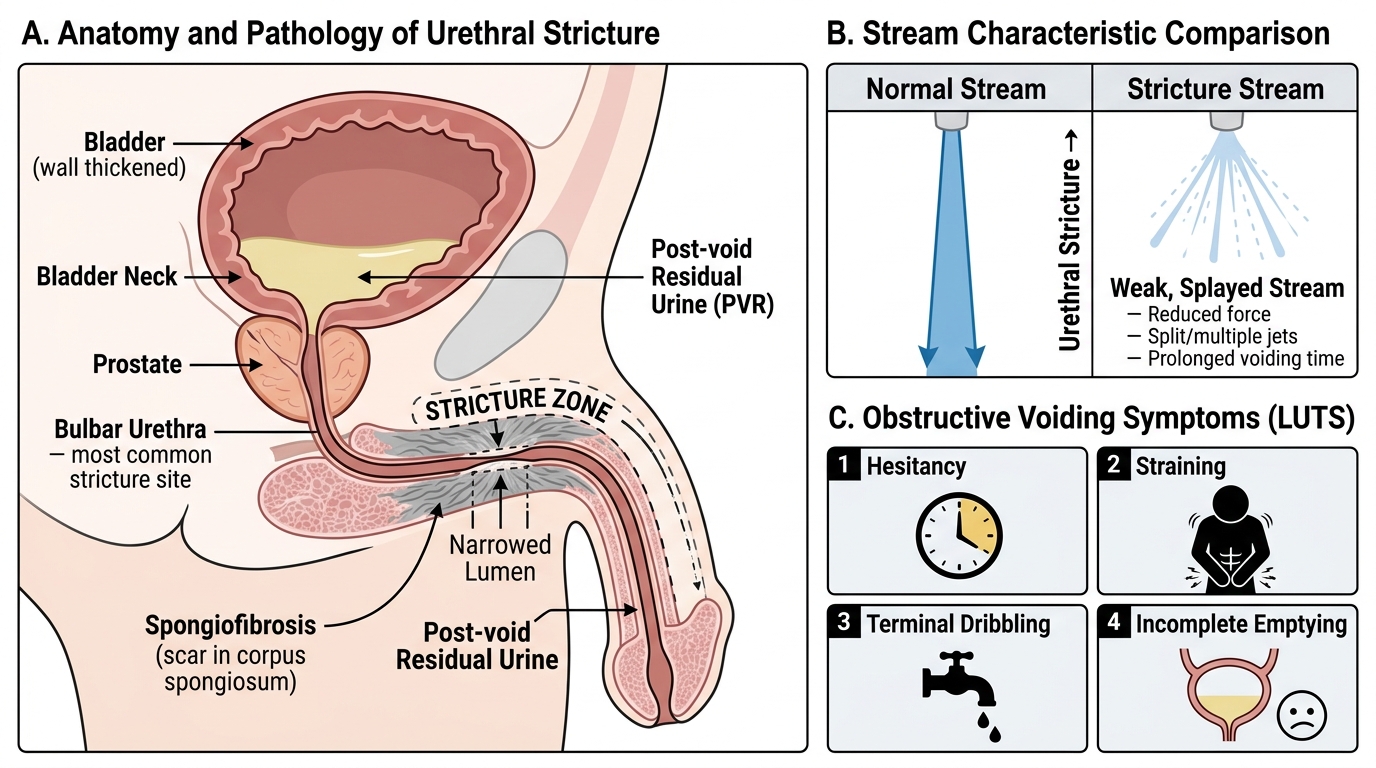
Urethral Stricture: Obstructive LUTS, Stream Pattern, and Pathological Anatomy
- Voiding symptoms: weak/poor-force stream, splaying or spraying of the stream, hesitancy, straining, prolonged voiding, terminal dribbling, sense of incomplete emptying.
- Complications: recurrent UTI, post-void residual and stones, acute/chronic retention, periurethral abscess, urethral fistula, and back-pressure renal change.
- History pointers to cause: straddle/perineal trauma, pelvic fracture, prior catheterisation/instrumentation/TURP, previous urethral infection or discharge.
Anatomy, Aetiology and the Pathology of Spongiofibrosis
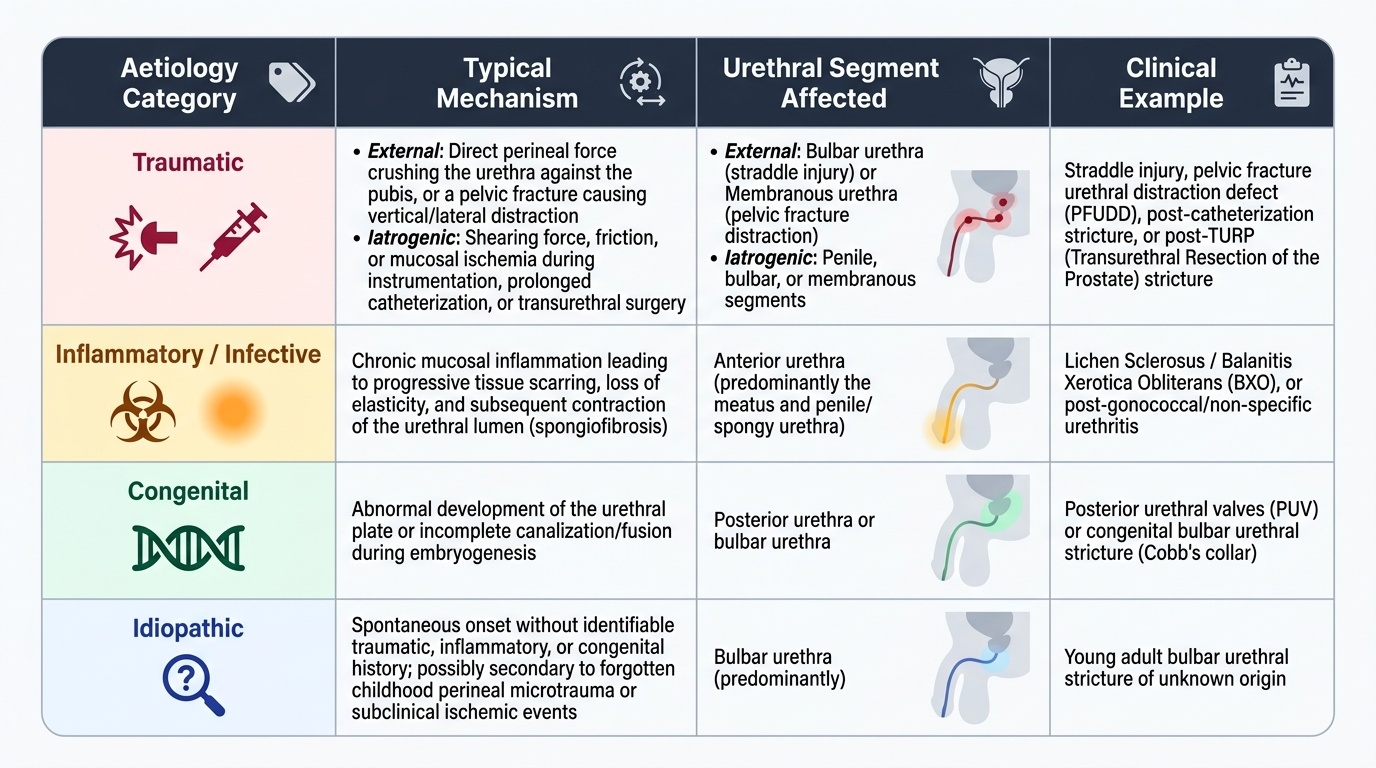
Understanding stricture means joining its pathology to its anatomy, because where a stricture sits and how it formed predict both its behaviour and its treatment. The pathological lesion is spongiofibrosis — fibrous scarring of the urethral epithelium and, crucially, of the surrounding corpus spongiosum of the anterior urethra. This scar contracts and narrows the lumen into a rigid, non-distensible segment; the depth and length of the spongiofibrosis, not merely the calibre of the lumen, determine how the stricture will respond to treatment. Anatomically it is essential to separate anterior from posterior strictures. The anterior urethra (penile and bulbar, within the corpus spongiosum) is the site of most strictures, and the bulbar urethra is the single commonest location, because it is the segment most exposed to blunt perineal force. The posterior urethra (membranous and prostatic) is affected differently: the membranous urethra is torn or distracted in pelvic-fracture urethral injury, healing as a dense scar or a distraction defect rather than a simple narrowing. Aetiologically, trauma is the major cause in modern practice and has two faces — external trauma (a straddle/perineal injury crushing the bulbar urethra against the pubis, or a pelvic fracture distracting the membranous urethra) and iatrogenic trauma from traumatic catheterisation, instrumentation, transurethral resection of the prostate (TURP) or a prolonged indwelling catheter. The second group is inflammatory/infective: post-inflammatory stricture after gonococcal or non-specific urethritis (historically common, now much reduced by antibiotics) and lichen sclerosus / balanitis xerotica obliterans (BXO), which scars the meatus and anterior urethra. The remainder are congenital or idiopathic.
Provided image
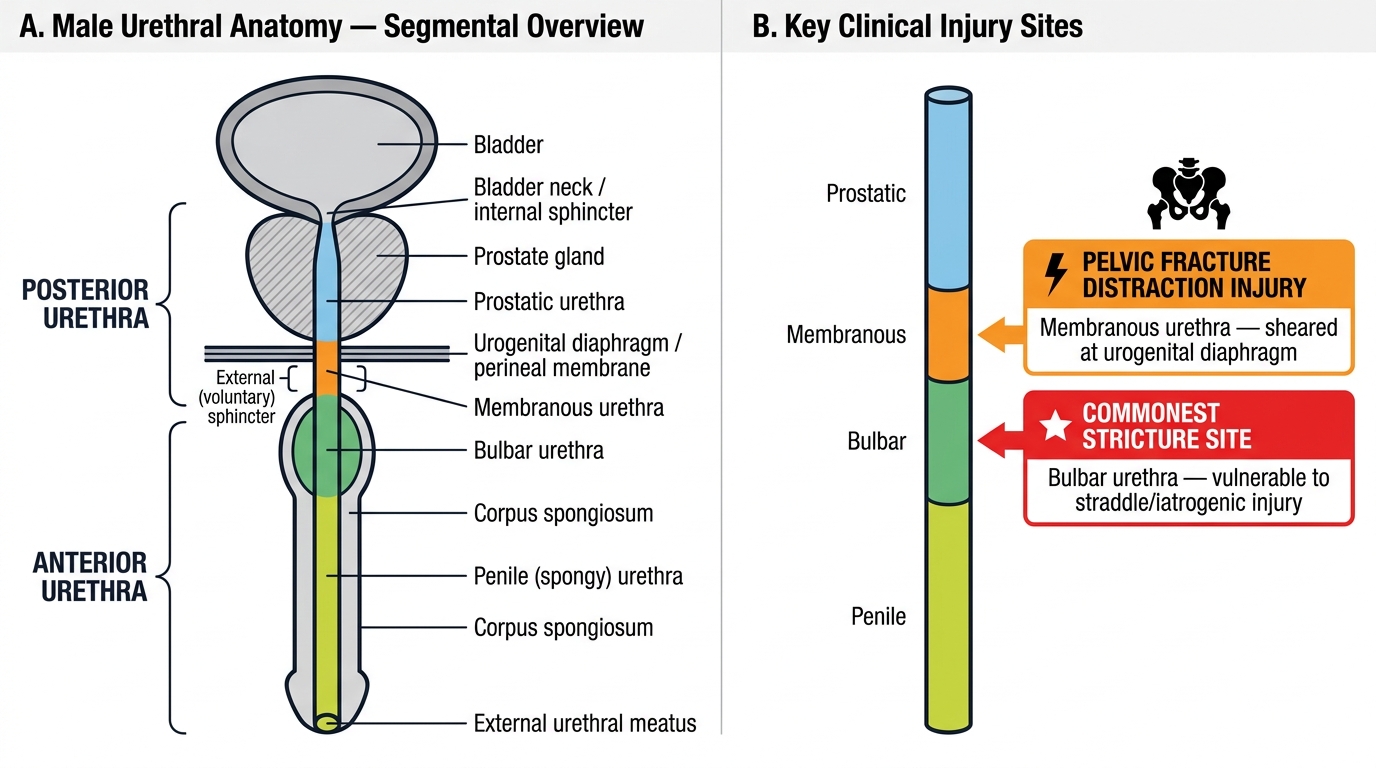
Male Urethral Segmental Anatomy and Key Clinical Injury Sites
| Aetiology | Typical mechanism | Segment affected | Example |
|---|---|---|---|
| Traumatic (external) | Straddle/perineal blunt force; pelvic fracture | Bulbar (straddle); membranous (pelvic fracture) | Fall astride; road-traffic pelvic fracture |
| Traumatic (iatrogenic) | Catheter/instrument/endoscopic injury | Any; often bulbar/penile | Traumatic catheterisation, TURP, prolonged catheter |
| Inflammatory/infective | Post-urethritis scarring; lichen sclerosus (BXO) | Anterior; meatal/penile (BXO) | Post-gonococcal stricture; BXO meatal stenosis |
| Congenital / idiopathic | Developmental or unknown | Variable | Congenital bulbar stricture; idiopathic |
SELF-CHECK
A young man develops a urethral stricture after falling astride a metal bar. Which urethral segment is most likely affected, and what is the underlying pathological process?
A. Prostatic urethra; benign prostatic hyperplasia
B. Bulbar (anterior) urethra; spongiofibrosis
C. Membranous urethra; detrusor overactivity
D. Penile urethra; lichen sclerosus
Reveal Answer
Answer: B. Bulbar (anterior) urethra; spongiofibrosis
A straddle (perineal) injury crushes the bulbar urethra against the inferior pubis, and the bulbar segment is the commonest site of anterior urethral stricture. The pathological substrate is spongiofibrosis — scarring of the urethral lining and the surrounding corpus spongiosum — which produces a rigid, non-distensible narrowing. Pelvic fractures, by contrast, distract the membranous (posterior) urethra.
Examination and Investigation of the Stricture
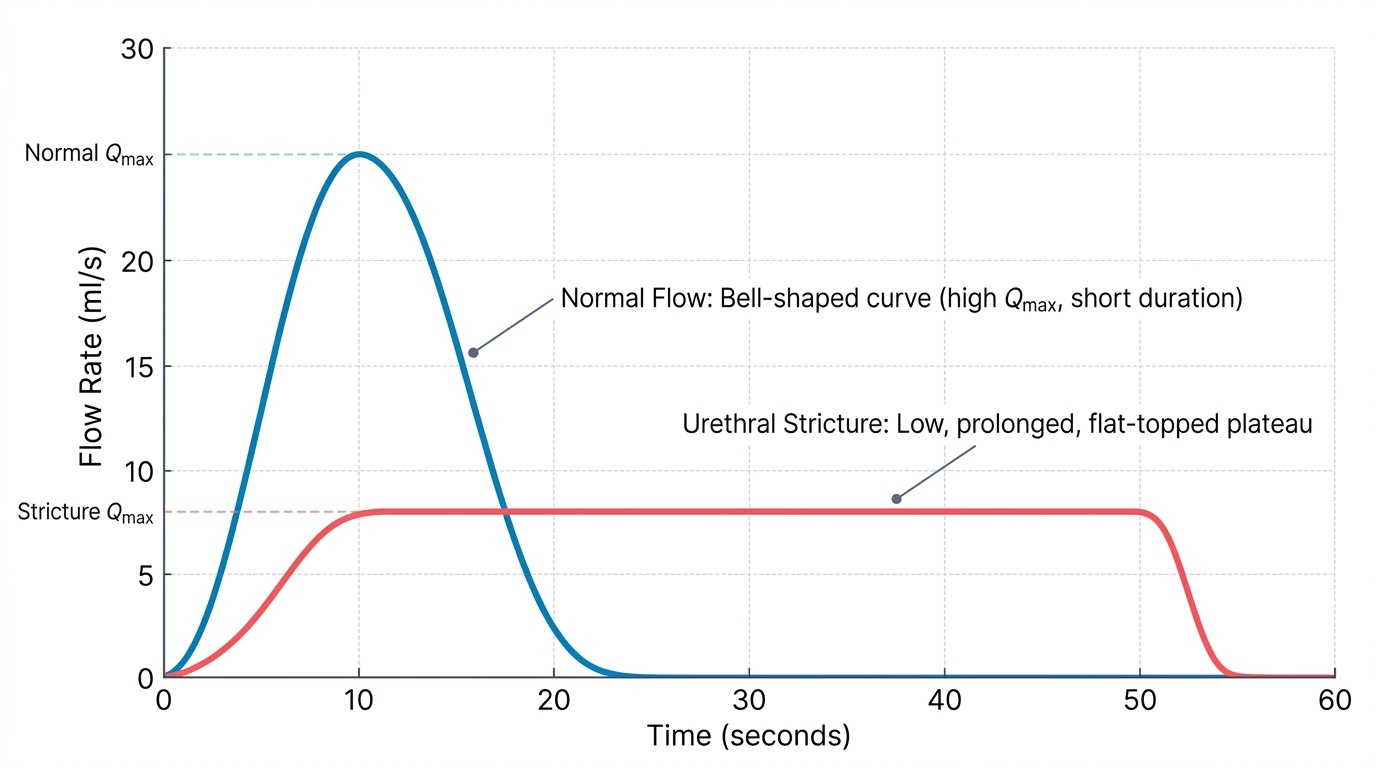
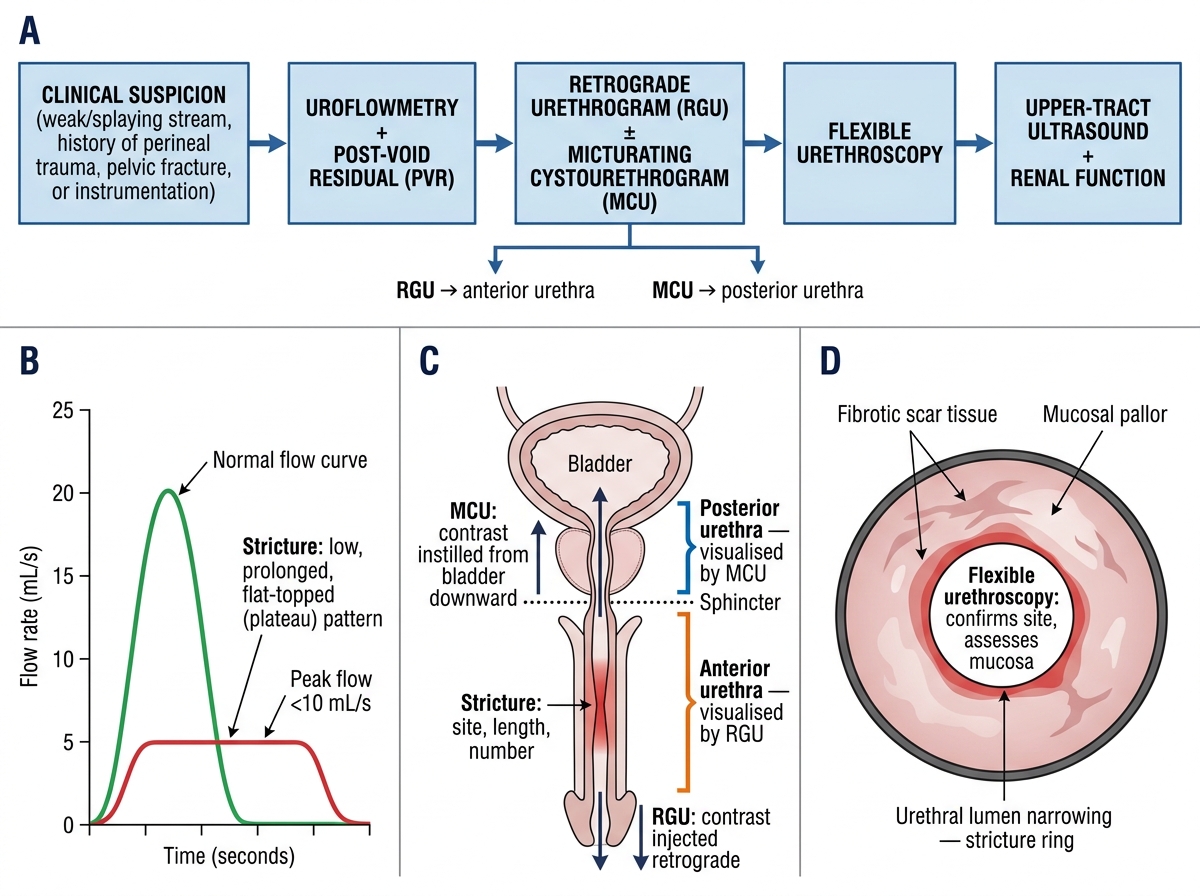
Examination is often unremarkable in a simple stricture, but it should still be systematic. Inspect the external meatus for stenosis and for the pale, scarred changes of lichen sclerosus / BXO; palpate the penile urethra along its length for a thickened, indurated cord that may mark the strictured segment; examine the perineum and scrotum for sinuses, an abscess or the multiple discharging tracks of a watering-can perineum; and palpate the abdomen for a distended, chronically retained bladder. The diagnosis, however, is confirmed and mapped by investigation, and the order is logical. Uroflowmetry is a simple, non-invasive screen: a stricture characteristically gives a low, prolonged, plateau (flat-topped, "box-shaped") flow curve rather than the normal bell shape, because the fixed narrowing caps the maximum flow regardless of detrusor effort. The post-void residual volume, measured by ultrasound, quantifies incomplete emptying and the obstructive burden. The single most important imaging study is the retrograde urethrogram (RGU), in which contrast is injected per meatum to outline the anterior urethra and reveal the site, length and number of strictures; it is combined with a micturating (voiding) cystourethrogram (MCU) — contrast voided after bladder filling — to display the posterior urethra above a tight or complete stricture, so that the two studies together map the whole urethra across the lesion. Flexible urethroscopy/cystoscopy allows direct inspection where the anatomy is unclear, and renal function tests with upper-tract ultrasound assess any back-pressure damage. Together these answer the two questions that drive treatment: where is the stricture, and how long and dense is it?
Provided image
Investigation Pathway for Suspected Urethral Stricture
- Uroflowmetry: low, prolonged, plateau (flat-topped/box-shaped) curve — the screening signature of stricture.
- RGU ± MCU: the key imaging — RGU outlines the anterior urethra and the stricture (site, length, number); MCU shows the posterior urethra above the lesion.
- Adjuncts: post-void residual (ultrasound), flexible urethroscopy, renal function and upper-tract ultrasound for back-pressure.
CLINICAL PEARL
Do not treat a young man's weak, splaying stream as if it were prostatic obstruction — alpha-blockers and 5-alpha-reductase inhibitors do nothing to a fixed scar. The age, the splayed stream and any history of perineal trauma, pelvic fracture or past instrumentation should send you to a retrograde urethrogram, not a prostate prescription. Equally, never force a catheter or an instrument through a tight stricture: blind, forceful passage creates a false passage and worsens the scar, turning a treatable short stricture into a complex one. When a man with a known stricture goes into acute retention and a catheter will not pass atraumatically, the safe answer is a suprapubic catheter, not repeated forceful attempts.