Page 11 of 26
SU29.11 | Urethral Strictures — SDL Guide (Part 2)
Surgical Management by Length and Site
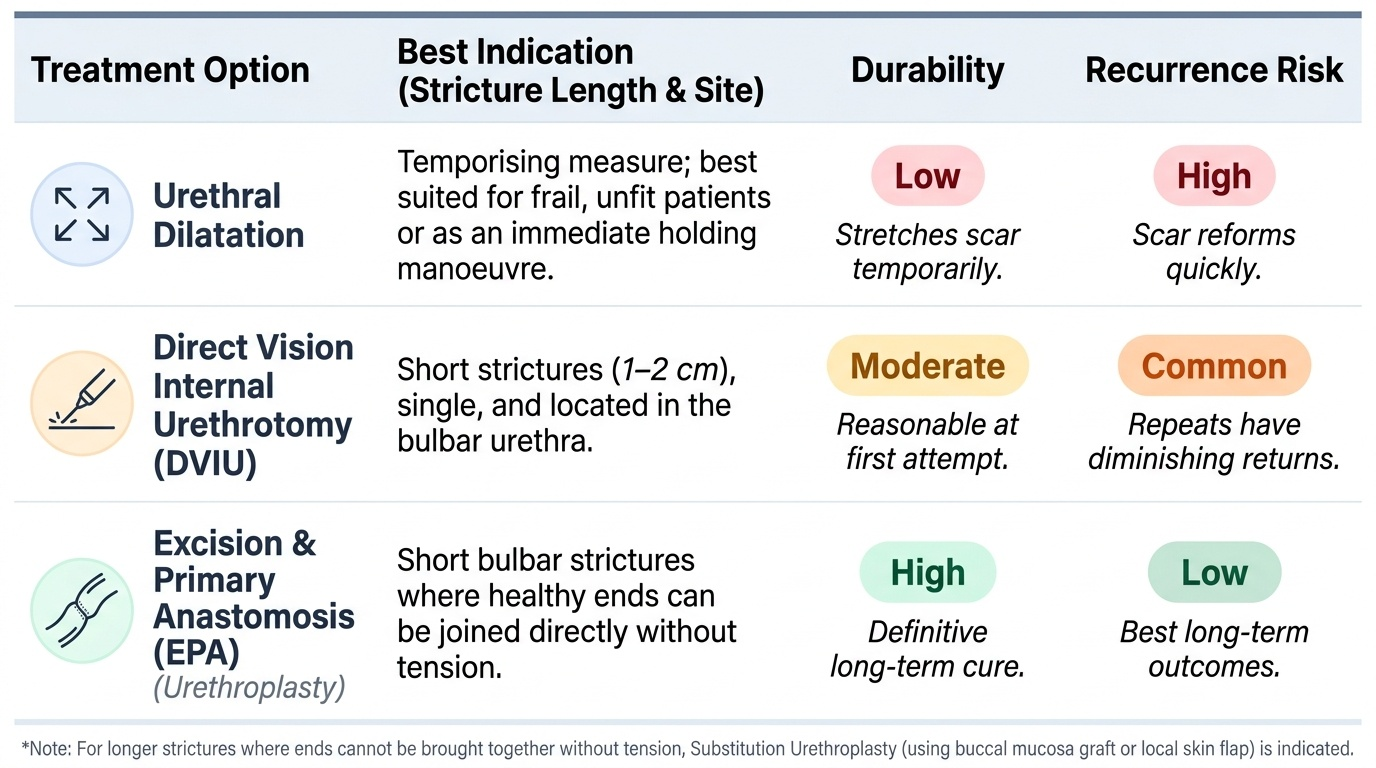
Management is chosen by the length, density, site and number of the stricture, and the central principle is that a short stricture and a long stricture are different problems. The least invasive options buy time but rarely cure. Urethral dilatation stretches and splits the scar with graduated bougies or balloons; it is simple and useful as a temporising measure, but the scar reforms and recurrence is high, so it is a holding manoeuvre rather than a definitive answer. Direct vision internal urethrotomy (DVIU) — also called optical internal urethrotomy — incises the stricture endoscopically under direct vision (an Otis urethrotome may be used for some anterior strictures); it works best for a short (<1-2 cm), single, bulbar stricture and gives a reasonable result at the first attempt, but recurrence is common and repeated urethrotomies have diminishing returns and progressively damage the urethra. The definitive, best-long-term-outcome operation is urethroplasty, an open reconstruction whose technique is itself chosen by length: for a short bulbar stricture, the scarred segment is excised and the healthy ends joined directly — excision and primary anastomosis (EPA); for a longer stricture where the ends cannot be brought together without tension, the lumen is augmented or replaced by substitution urethroplasty using a buccal mucosa graft (the graft of choice for its wet, elastic, robust epithelium and low donor-site morbidity) or a local skin flap. Finally, when a man presents in acute retention and a urethral catheter cannot be passed, the immediate, safe step is a suprapubic catheter to drain the bladder before any definitive plan. Whatever is done, the patient must be counselled that strictures recur and that long-term follow-up — with symptom review and uroflowmetry — is part of the contract of care.
Provided image
| Option | Best indication | Durability | Recurrence risk |
|---|---|---|---|
| Dilatation | Temporising; frail/unfit patient | Low | High (scar reforms) |
| DVIU (optical internal urethrotomy) | Short (<1-2 cm) single bulbar stricture | Moderate at first attempt | Common; repeat attempts fail |
| Excision + primary anastomosis (urethroplasty) | Short bulbar stricture | High (definitive) | Low |
| Substitution urethroplasty (buccal mucosa graft/flap) | Longer or recurrent stricture | High (definitive) | Low |
| Suprapubic catheter | Acute retention when urethral access impossible | Temporary drainage | n/a (bridge to definitive care) |
Check Your Understanding
Bring the threads together by reasoning back through the young man in the hook. His slow, progressive, splaying, straining stream is the classic obstructive picture of a stricture; his forgotten straddle injury two years earlier points to a bulbar (anterior) stricture from spongiofibrosis; and his episode of fever and retention warns of the complications of stagnant residual urine. The correct next step is not a prostate prescription but a retrograde urethrogram to map the site, length and number of strictures, supported by uroflowmetry (expect a flat-topped curve) and a post-void residual. The treatment then follows the map: if the RGU shows a short single bulbar stricture, a DVIU or, better for durability, an excision-and-primary-anastomosis urethroplasty is appropriate; if it shows a longer stricture, a substitution urethroplasty with a buccal mucosa graft is the definitive choice. Use the hook to self-test the four competencies this module covers. First, can you list the obstructive symptoms and complications that should make you suspect a stricture? Second, can you explain spongiofibrosis and name the commonest site and the major cause? Third, can you state why the retrograde urethrogram is the key investigation and what a stricture does to the uroflow curve? Fourth, can you match dilatation, DVIU and the two urethroplasty techniques to stricture length? The questions that follow check exactly these links.
SELF-CHECK
Which statement about the management of urethral stricture is correct?
A. Repeated urethral dilatation reliably cures most strictures and is the definitive treatment.
B. Direct vision internal urethrotomy is best suited to long, dense, recurrent strictures.
C. Urethroplasty is the definitive treatment; excision-and-primary-anastomosis suits short bulbar strictures and a buccal mucosa graft is used for longer strictures.
D. A man in acute retention with an impassable stricture should have a urethral catheter forced through under sedation.
Reveal Answer
Answer: C. Urethroplasty is the definitive treatment; excision-and-primary-anastomosis suits short bulbar strictures and a buccal mucosa graft is used for longer strictures.
Urethroplasty gives the best long-term success and is the definitive treatment: a short bulbar stricture is treated by excision and primary anastomosis, while a longer stricture needs substitution urethroplasty, typically with a buccal mucosa graft. Dilatation is only temporising (high recurrence); DVIU suits SHORT (<1-2 cm) single bulbar strictures, not long dense ones; and an impassable stricture in acute retention is managed with a suprapubic catheter, never by forcing a urethral catheter (which creates a false passage).