Page 4 of 11
SU3.2-3 | Transfusion Observation and Donation Counselling — SDL Guide
Learning Objectives
- Perform the safe-transfusion bedside check, including positive patient identification against the compatibility label, and observe a transfusion safely (SU3.2).
- Describe the schedule of pre-, intra- and post-transfusion observations and recognise the early bedside features of a transfusion reaction (SU3.2).
- Counsel a patient and family before a transfusion — covering indication, benefits, risks, alternatives and informed consent (SU3.3).
- Counsel a prospective donor for voluntary blood donation — covering eligibility and deferral, the steps of donation, post-donation care, and the basis of a safe voluntary blood supply (SU3.3).
INSTRUCTIONS
Giving blood safely is as much a bedside skill as a laboratory one. The single most lethal transfusion error — an ABO-incompatible reaction — almost always begins not in the blood bank but at the bedside, when the wrong unit reaches the wrong patient. This module turns the science of the previous module into practice: how to identify the patient and check the unit, how to observe a transfusion so a reaction is caught in its first minutes, how to obtain valid consent, and how to counsel a healthy person to become a safe voluntary donor. These are skills you will use, and supervise, throughout your career.
References
- Bailey & Love's Short Practice of Surgery, Transfusion of Blood and Blood Products chapter (textbook)
- SRB's Manual of Surgery, Blood Transfusion and Blood Banking (textbook)
- National Blood Transfusion Council (NBTC), Standards for Blood Banks & Blood Transfusion Services (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
On a busy surgical ward two patients in adjacent beds are both due for transfusion. A nurse collects a unit, walks to the bedside, and is about to connect it when the house officer stops to do the bedside check properly: she asks the patient to state his full name and date of birth, checks the wristband, and compares every detail against the compatibility label on the unit and the patient's identity. The name matches — but the hospital number does not. The unit was crossmatched for the man in the next bed. That ten-second check, performed correctly, has just prevented a fatal ABO-incompatible haemolytic reaction. No crossmatch in the laboratory could have caught this error; only the person at the bedside could. This module is about that person, and about the conversations — consent and donation counselling — that make the whole transfusion service safe and sustainable.
WHY THIS MATTERS
Observing a transfusion and counselling for blood are core competencies you will perform from your first clinical posting. The reason they matter so much is that the most catastrophic transfusion outcomes are preventable at exactly these two points. The commonest cause of a fatal haemolytic reaction is a patient-identification error — a 'wrong blood in tube' or a wrong-unit-to-wrong-patient slip — that only a disciplined bedside check can intercept, and the early minutes of observation are when a developing reaction can still be stopped. Equally, a safe and adequate blood supply depends on counselling: a patient who understands why blood is needed, its benefits and risks and the alternatives can give genuine informed consent, and a healthy person who is properly counselled becomes a voluntary, non-remunerated, repeat donor — the safest possible source of blood. Get these skills right and you prevent the errors that kill, respect patients' autonomy, and help sustain the donor pool that every surgical patient depends on.
RECALL
Before going further, recall a few things from earlier learning. First, the ABO and Rh compatibility you have just studied: the reason patient identity matters so much is that an ABO-incompatible unit triggers immediate IgM-mediated intravascular haemolysis, the most dangerous reaction of all. Second, the early features of the common transfusion reactions from the previous module — fever and rigors, urticaria, breathlessness, loin or back pain, hypotension — because observation is simply watching for these. Third, the principles of informed consent you met in medical ethics: a valid consent requires a competent patient, adequate disclosure of the nature, benefits, risks and alternatives of the procedure, and a voluntary, uncoerced decision. Keep these three ideas in mind — safe observation and good counselling are these familiar principles applied carefully at the bedside.
The Bedside Stakes: Why Observation and Counselling Are Skills
It is tempting to think of transfusion safety as something achieved in the blood bank — by grouping, antibody screening and crossmatching — but the evidence is clear that the bedside is where most preventable harm is decided. The great majority of serious, and nearly all fatal, ABO-incompatible reactions arise not from a laboratory failure but from a patient-identification error: a sample taken from the wrong patient and labelled with another's details ('wrong blood in tube'), or a correctly crossmatched unit connected to the wrong person. This is why observing a transfusion is a genuine clinical skill (SU3.2), not a passive task: it begins with a rigorous identity check that is the final barrier against a fatal error, and continues with structured monitoring that catches a developing reaction in the minutes when stopping the transfusion still matters. The second skill, counselling (SU3.3), underpins safety from a different direction. Before a transfusion, the patient and family deserve — and the law and ethics require — a clear explanation of why blood is needed, what it will achieve, what can go wrong, and what alternatives exist, so that consent is genuinely informed. And the entire supply rests on voluntary, non-remunerated donation, which counselling encourages and sustains; voluntary repeat donors carry the lowest risk of transmitting infection, so persuading a healthy, eligible person to donate is itself an act of patient safety. Together, careful observation and honest counselling convert the science of transfusion into safe, ethical practice.
Governing Principles of Safe Transfusion and Valid Consent
Three sets of principles govern these skills. The first is the right-patient/right-unit principle that runs as an unbroken chain from sampling to administration: the blood sample must be taken from, and labelled at, the bedside of the correctly identified patient; the laboratory performs grouping and a crossmatch (or a group-and-screen with electronic issue) to confirm compatibility; and, crucially, the bedside identity check immediately before connecting the unit re-verifies that this unit, on its compatibility label, belongs to this patient. Every link can be undone by the next, so the bedside check is the final and most important safeguard. The second is the principle of valid informed consent: consent for transfusion requires a competent patient who has received adequate information — the indication for transfusion, its expected benefit, the material risks (including reactions and, rarely, transmitted infection), and the available alternatives (such as iron, optimisation of anaemia, or, where appropriate, cell salvage) — and who decides voluntarily. The third governs donation: a safe blood supply is built on voluntary non-remunerated repeat donors, because the absence of payment removes the incentive to conceal risk factors and repeat testing lowers residual risk. Donor eligibility protects both donor and recipient: typical Indian criteria include age 18–65 years, body weight of at least 45 kg, a haemoglobin of at least 12.5 g/dL, and an inter-donation interval of three months for whole blood, with deferral for anaemia, recent illness or fever, recent tattooing or piercing, high-risk behaviour, pregnancy or recent childbirth, and certain medications or recent vaccination. Every donation is screened for the mandatory transfusion-transmissible infections — HIV, hepatitis B, hepatitis C, syphilis and malaria.
- Right-patient/right-unit chain: correct bedside sampling → laboratory grouping & crossmatch → bedside identity check before connecting (the final barrier).
- Valid consent for transfusion: competent patient + disclosure of indication, benefit, risks and alternatives + voluntary decision.
- Donation principles: voluntary, non-remunerated, repeat donation is safest; eligibility (age 18–65, ≥45 kg, Hb ≥12.5 g/dL, 3-month interval) + mandatory TTI screening (HIV, HBV, HCV, syphilis, malaria).
Observing a Transfusion: The Step-by-Step Procedure
Observing a transfusion follows an ordered, repeatable procedure, and performing it the same way every time is what makes it safe. It begins before the unit is hung: confirm that valid consent and a written prescription exist, and that the unit is the correct component for this patient. Then carry out the positive patient identification and bedside check — the single most important step. Ask the conscious patient to state their full name and date of birth (do not ask leading questions such as 'are you Mr X?'), check the identity wristband, and match every identifier — name, hospital number, date of birth — against the compatibility label attached to the unit and the accompanying documentation; also check the blood group, the unit's donation number and its expiry, and inspect the bag for discolouration, clots or leaks. Any discrepancy means the unit is not given. Record a full set of baseline observations — temperature, pulse, blood pressure, respiratory rate and oxygen saturation — immediately before starting, because a reaction is recognised as a change from this baseline. Start the transfusion slowly and observe the patient especially closely for the first 15 minutes, when the most dangerous reactions (acute haemolytic, severe allergic and bacterial sepsis) typically declare themselves; repeat the observations at about 15 minutes, then periodically through the transfusion and again at completion, and complete each unit within four hours of its leaving controlled storage. Throughout, stay alert for the early warning features. If a reaction is suspected, the immediate action is always the same: stop the transfusion at once, keep the intravenous line open with saline, recheck the patient's identity against the unit, assess and support airway, breathing and circulation, and call for senior help — then return the unit and a fresh sample to the laboratory.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
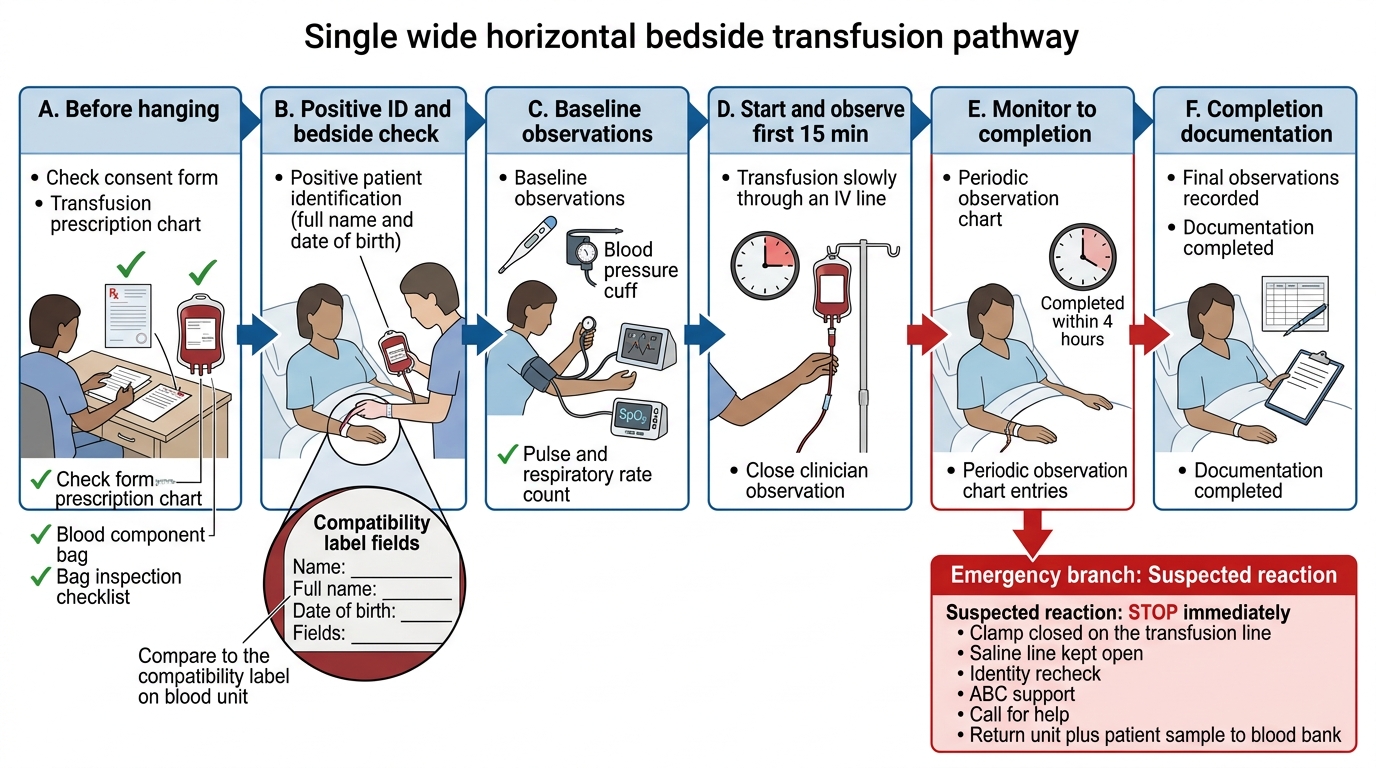
Safe Bedside Transfusion Procedure
- Before hanging: valid consent + prescription; correct component; inspect the bag.
- Positive ID / bedside check: patient states name & DOB; match wristband to the compatibility label (name, hospital number, DOB, group, donation number, expiry).
- Baseline observations: temperature, pulse, BP, respiratory rate, SpO₂ before starting.
- Monitor: start slowly, watch closely for the first 15 minutes, then periodically and at completion; finish within 4 hours.
- If a reaction is suspected: STOP the transfusion, keep the line open with saline, recheck identity, support ABC, call for help, return unit and sample.
SELF-CHECK
While checking a patient before transfusion, the safest way to confirm identity is to:
A. Ask 'Are you Mr Sharma?' and proceed if the patient nods
B. Ask the patient to state their full name and date of birth, then match the wristband against the compatibility label on the unit
C. Check the bed number against the prescription chart
D. Confirm the blood group verbally with the nurse who collected the unit
Reveal Answer
Answer: B. Ask the patient to state their full name and date of birth, then match the wristband against the compatibility label on the unit
Positive patient identification means the patient actively states their full name and date of birth (open questions, not leading ones), which are then matched against the identity wristband AND the compatibility label on the unit. Leading questions, bed numbers and verbal-only checks are unreliable and are exactly how wrong-patient/wrong-unit errors — the commonest cause of fatal haemolytic reactions — slip through.