Page 5 of 11
SU3.2-3 | Transfusion Observation and Donation Counselling — SDL Guide (Part 2)
Interpreting What You Observe at the Bedside
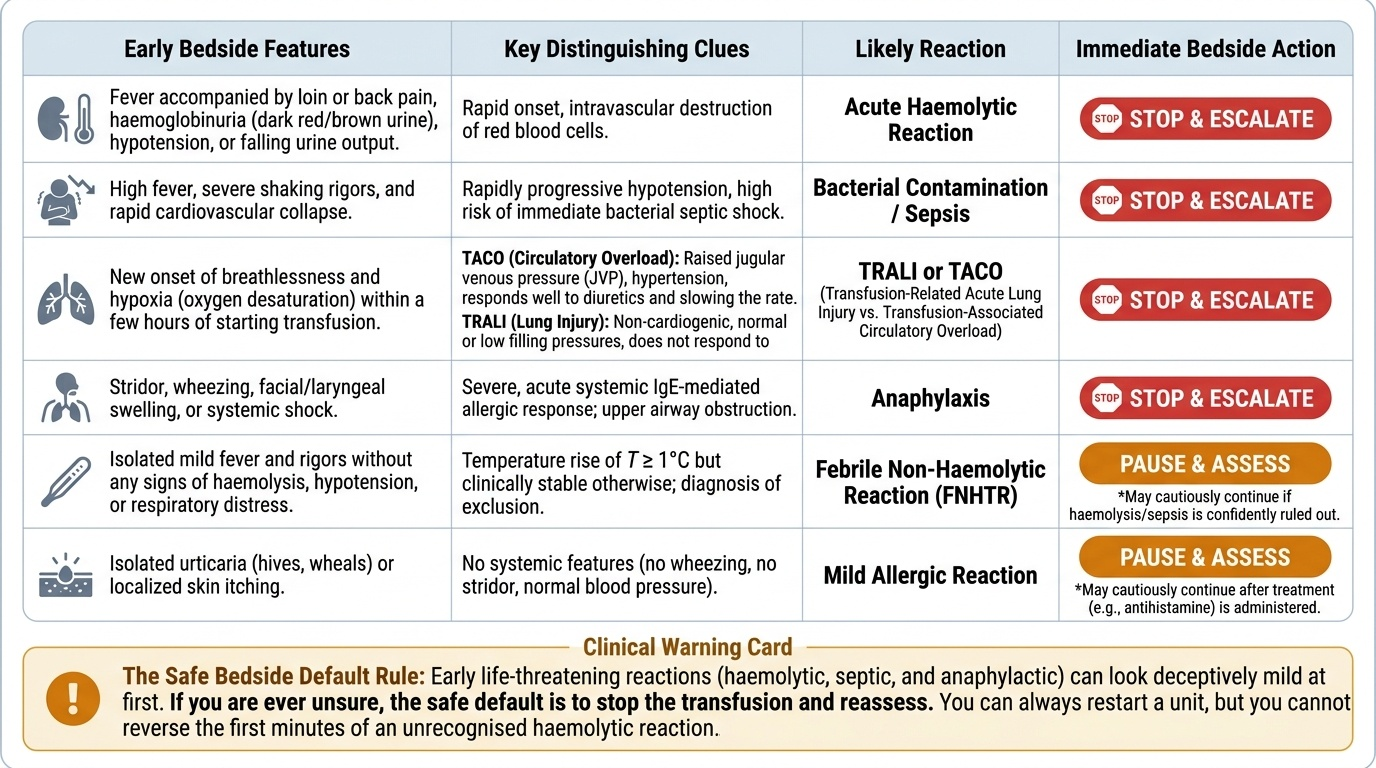
Observation is only useful if you can interpret what you see and decide between continuing with caution and stopping and escalating. The interpretation rests on three things: the timing relative to starting the unit, the pattern of features, and the trajectory — whether the patient is stable or deteriorating. Some features are clear danger signals demanding the transfusion be stopped immediately: fever with loin or back pain, haemoglobinuria, hypotension or a falling urine output points to an acute haemolytic reaction; high fever with rigors and rapid collapse suggests bacterial contamination and septic shock; new breathlessness with hypoxia within a few hours raises TRALI; and stridor, wheeze, facial swelling or shock indicate anaphylaxis. Other features are usually less sinister but still need pausing and assessment: an isolated mild fever with rigors but no haemolysis suggests a febrile non-haemolytic reaction, and isolated urticaria or itch suggests a mild allergic reaction — both may allow cautious continuation after treatment once a dangerous reaction has been excluded. A critical interpretive trap is distinguishing TACO from TRALI when a patient becomes breathless: TACO is circulatory overload, with a raised jugular venous pressure, hypertension and a good response to slowing the transfusion and giving a diuretic, whereas TRALI is non-cardiogenic, with normal or low filling pressures. Because early haemolytic, septic and anaphylactic reactions can look deceptively mild at first, the safe default whenever you are unsure is to stop the transfusion and reassess rather than press on — you can always restart a unit, but you cannot reverse the first minutes of an unrecognised haemolytic reaction.
Provided image
- Stop and escalate: fever + loin pain/haemoglobinuria/hypotension (acute haemolytic); high fever + rigors + collapse (sepsis); breathlessness + hypoxia <6 h (TRALI); stridor/wheeze/swelling/shock (anaphylaxis).
- Pause, assess, often continue with caution: isolated mild fever/rigors without haemolysis (FNHTR); isolated urticaria/itch (mild allergic).
- TACO vs TRALI: TACO = raised JVP, hypertension, diuretic-responsive (overload); TRALI = non-cardiogenic, normal filling pressures.
- When in doubt: stop and reassess — the safe default.
Counselling for Transfusion and for Voluntary Donation
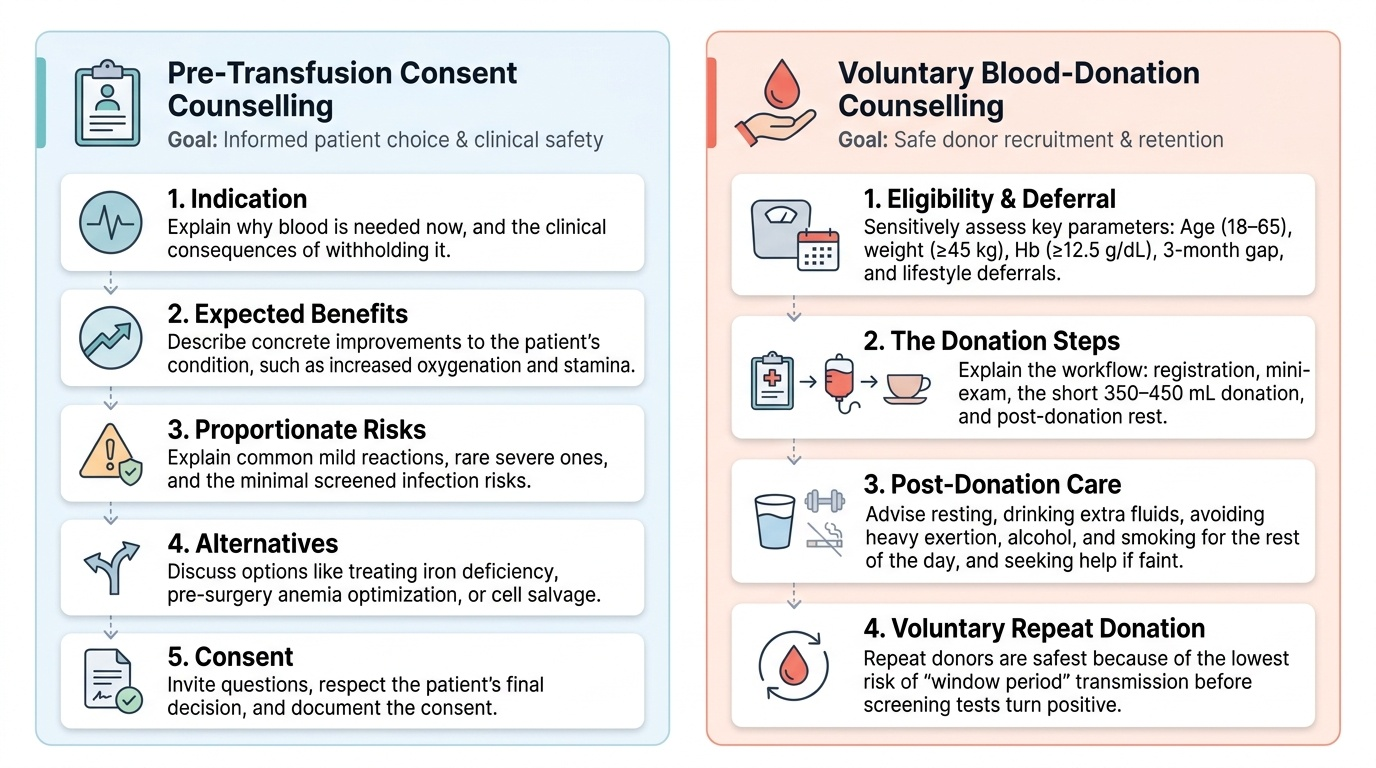
Counselling is a structured conversation, and rehearsing its structure makes it reliable under pressure. For pre-transfusion consent counselling, work through a clear sequence in language the patient and family understand. Explain the indication — why this patient needs blood now and what is likely to happen without it; describe the expected benefit in concrete terms; disclose the risks honestly but proportionately — the common, usually mild reactions, the rare serious ones, and the very small, screened residual risk of transmitted infection; and offer the alternatives where they exist, such as treating iron deficiency, optimising anaemia before elective surgery, or intra-operative cell salvage. Then invite questions, confirm understanding, respect a competent patient's right to accept or decline, and document the consent. For voluntary blood-donation counselling, the aim is to recruit and reassure a safe donor. Confirm eligibility and screen for deferral sensitively — age 18–65, weight at least 45 kg, haemoglobin at least 12.5 g/dL, an interval of three months since the last whole-blood donation, and the absence of recent illness, high-risk behaviour, recent tattoo or piercing, pregnancy or relevant medication. Walk the donor through the steps of donation — registration and consent, a confidential health questionnaire and mini-examination, the donation itself of about 350–450 mL taking only a few minutes, and a short rest with refreshment afterwards — and reassure them it is safe and the body replaces the donated blood. Give clear post-donation advice: rest briefly, take extra fluids, avoid heavy exertion, alcohol and smoking for the rest of the day, and seek help if they feel faint. Finally, encourage voluntary, non-remunerated, repeat donation and explain, simply, why it gives the safest blood — repeat voluntary donors have the lowest risk of transmitting infection during the window period, the early interval when a newly infected donor can be infectious before screening tests turn positive.
Provided image
- Consent counselling (before transfusion): indication → benefit → risks (common mild, rare serious, residual TTI) → alternatives → invite questions → document consent.
- Donation counselling: eligibility & deferral screen → steps of donation → safety reassurance → post-donation care → encourage voluntary repeat donation.
- Why voluntary repeat donors are safest: no incentive to conceal risk; repeat testing minimises window-period residual risk.
Check Your Understanding
Consolidate these skills by rehearsing them as you would perform them, not by reciting facts. Picture yourself at the bedside about to start a transfusion and walk through the procedure aloud: confirm consent and prescription, ask the conscious patient to state their full name and date of birth, match the wristband against the compatibility label on the unit, record baseline observations, and plan to watch closely for the first 15 minutes — and remember that a single mismatched identifier means you do not give the unit. Now rehearse the stop-the-transfusion sequence: at the first sign of a serious reaction you stop the transfusion, keep the line open with saline, recheck identity, support airway, breathing and circulation, call for help, and return the unit and a sample to the laboratory. Then test your interpretation: place fever-with-loin-pain-and-haemoglobinuria, isolated urticaria, breathlessness-with-raised-JVP and breathlessness-with-normal-filling-pressures into stop-and-escalate or continue-with-caution. Finally, rehearse a counselling encounter: in your own words, take a patient through indication, benefit, risks and alternatives to valid consent, and take a healthy visitor through eligibility, the donation steps, post-donation care and why voluntary repeat donation gives the safest blood. If you can perform these three rehearsals fluently, you have met the competency.
CLINICAL PEARL
Positive identification means the patient does the talking. Always ask an able patient to state their own full name and date of birth and then match those details to the wristband AND the compatibility label on the unit — never ask 'Are you Mr X?', because a frightened, drowsy or hard-of-hearing patient may simply agree. This ten-second open-question check at the bedside is the final barrier against the wrong-patient/wrong-unit error that causes most fatal haemolytic reactions, and no laboratory crossmatch can substitute for it.
SELF-CHECK
A prospective voluntary blood donor asks why repeat voluntary donors are considered to give the safest blood. The best explanation is that:
A. Their blood contains more clotting factors than paid donors'
B. They are paid less so the blood costs less to collect
C. They have no incentive to conceal risk factors, and repeat screening minimises the residual 'window period' risk of transmitting infection
D. Voluntary donors are always group O and therefore universal donors
Reveal Answer
Answer: C. They have no incentive to conceal risk factors, and repeat screening minimises the residual 'window period' risk of transmitting infection
Voluntary, non-remunerated repeat donors are the safest source because, without payment, there is no incentive to conceal risk factors that would lead to deferral, and repeated screening over time minimises the residual risk from the window period — the early interval when a newly infected donor is infectious but screening tests are still negative. Donor blood group is unrelated to safety in this sense, payment is precisely what makes paid donation less safe, and clotting-factor content is not the issue.