Page 1 of 14
SU5.1-2 | Wound Healing and Wound Assessment — SDL Guide
Learning Objectives
- Describe the four overlapping phases of normal wound healing and the cells and mediators that drive each (SU5.1).
- Distinguish healing by primary, secondary and tertiary (delayed primary) intention and state when each applies (SU5.1).
- Enumerate the local and systemic factors that impair wound healing and explain the mechanism of each (SU5.1).
- Elicit, document and present a structured history and examination in a patient presenting with a wound (SU5.2).
INSTRUCTIONS
Every operation ends with a wound, and a great deal of trauma presents as one. Whether a wound heals cleanly in days or breaks down, becomes infected and lingers for weeks depends on biology the surgeon can read and on factors the surgeon can change. This module builds the basic-science foundation of wound healing — the phases, the modes of closure, and the local and systemic factors that derail them — and then turns to the bedside skill of taking and documenting a wound history. It underpins everything that follows on wound management and surgical infection.
References
- Bailey & Love's Short Practice of Surgery, Wound Healing and Wound Management chapter (textbook)
- SRB's Manual of Surgery, Wounds and Wound Healing (textbook)
- Sabiston Textbook of Surgery, Wound Healing (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients have the same operation on the same morning. The first, a fit 30-year-old, has a clean, dry incision that knits together in a week and leaves a thin pale line. The second, a 62-year-old with poorly controlled diabetes who smokes and is malnourished, develops a red, gaping, weeping wound that takes six weeks to close and leaves an ugly scar. The surgery was identical; the biology of healing was not. None of the second patient's troubles were random — every one of them traces to a phase of healing that stalled or a factor that impaired it. If you can read which phase a wound is in and which factors are working against it, you can predict trouble before it declares itself and act to prevent it.
WHY THIS MATTERS
Wound healing sits under every surgical decision. It explains why a clean sutured incision needs only a few days of protection while a contaminated open wound is deliberately left to granulate, why a diabetic or steroid-dependent patient is warned that their wound will be slow and fragile, and why nutrition, glycaemic control and stopping smoking are genuine surgical interventions and not afterthoughts. Get the model right and you choose the correct method of closure, anticipate which patients will struggle, and optimise the factors you can change. Get it wrong and you close a dirty wound that abscesses, miss the malnourished patient whose wound will dehisce, or fail to document a wound whose appearance later becomes a medico-legal question. This is foundational surgical science, examined directly and applied on every ward round.
RECALL
Before going further, recall three pieces of basic science you already know. First, haemostasis: when a vessel is injured, platelets adhere and aggregate to form a plug and the coagulation cascade lays down fibrin — the same process that will start every wound. Second, acute inflammation: injured tissue and activated macrophages release cytokines and growth factors that recruit neutrophils and then macrophages to clear debris and orchestrate repair. Third, collagen synthesis: fibroblasts make collagen, and the hydroxylation steps that cross-link it require vitamin C as a cofactor — which is why scurvy causes wounds to break down. Keep these three in mind: normal wound healing is essentially these familiar processes running in a coordinated, overlapping sequence.
Why Wound Healing Matters to the Surgeon
A wound is any breach in the normal structure and function of skin or underlying tissue, whether caused by trauma or made deliberately at operation. Wound healing is the orderly biological process by which the body restores the integrity of that injured tissue. For the surgeon this matters for a simple reason: every incision is a wound, and the surgeon's job does not end when the last suture is tied but when the wound has healed soundly. Healing is best understood not as a single event but as a programmed sequence of overlapping phases that is broadly predictable, proportional to the size and contamination of the wound, and — crucially — modifiable. Knowing its shape lets the surgeon choose the right method of closure, recognise when a wound is failing to progress, anticipate which patients will heal slowly, and intervene on the factors that can be changed. Sound understanding here prevents the two commonest avoidable disasters of surgical wounds: closing a wound that should have been left open, and failing to optimise a patient whose healing is doomed to fail. Importantly, healing can be helped: good perfusion, control of infection, removal of dead tissue and foreign material, adequate nutrition and control of diabetes all push a wound toward sound, timely repair.
The Four Phases of Normal Wound Healing
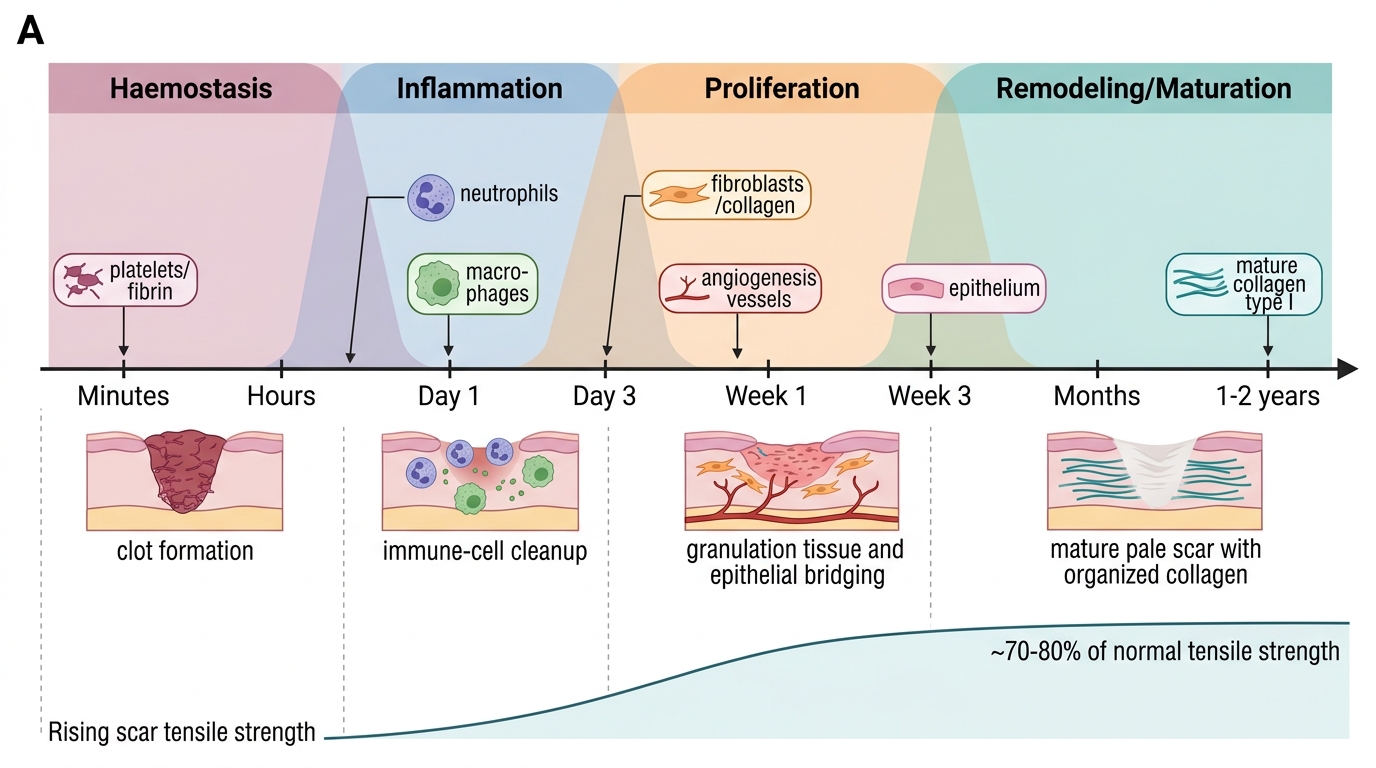
Normal wound healing proceeds through four phases that overlap in time rather than occurring as discrete steps. The first is haemostasis, beginning within seconds: vasoconstriction limits bleeding, platelets aggregate to form a plug, and the coagulation cascade lays down a fibrin clot that also acts as a provisional scaffold and a reservoir of growth factors. The second is the inflammatory phase, lasting from the first day to roughly day three to five: neutrophils arrive first to kill bacteria and clear debris, and are then succeeded by macrophages, the key orchestrating cell, which continue debridement and secrete the growth factors that drive the next phase. The third is the proliferative phase, from about day three to three weeks: fibroblasts synthesise collagen (initially weak type III), new capillaries grow in (angiogenesis), and together these form red, granular granulation tissue; meanwhile epithelial cells migrate across the surface (epithelialisation) and myofibroblasts begin wound contraction. The fourth is the remodeling (maturation) phase, which continues for months and up to one to two years: the disorganised type III collagen is gradually replaced by stronger, organised type I collagen, the scar becomes paler and flatter, and tensile strength rises — but a healed scar regains at most about 70 to 80 per cent of the original tissue's strength and never reaches 100 per cent.
Overlapping Phases of Wound Healing
- Haemostasis (seconds–minutes): vasoconstriction, platelet plug, fibrin clot as provisional scaffold.
- Inflammation (day 1 to ~3–5): neutrophils then macrophages clear debris and secrete growth factors; macrophage is the orchestrating cell.
- Proliferation (~day 3 to 3 weeks): fibroblasts and collagen, angiogenesis, granulation tissue, epithelialisation, contraction.
- Remodeling/maturation (weeks to ~1–2 years): type III collagen replaced by organised type I; scar matures; tensile strength rises to ~70–80% of normal.
Types of Healing: Primary, Secondary and Tertiary Intention
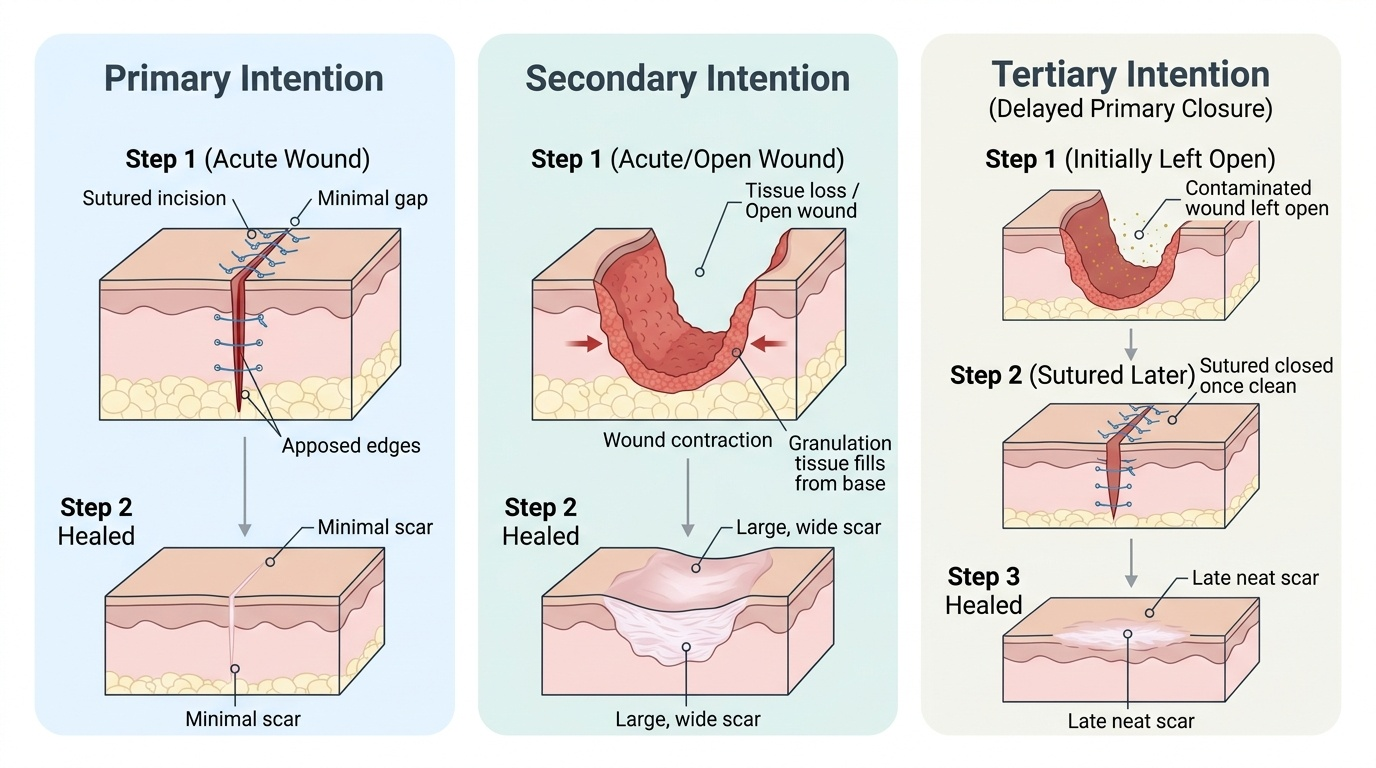
The same biological phases above can play out in three different ways depending on how the wound edges are managed, and naming the mode of healing is part of every operation note. Healing by primary intention occurs when a clean wound with minimal tissue loss has its edges brought together and held in apposition — the typical sutured surgical incision or a cleanly stitched laceration. Because the gap is small, there is little granulation tissue, healing is fast and the scar is neat. Healing by secondary intention occurs when a wound is left open — because there is tissue loss, contamination or infection that makes closure unsafe — and heals from the base upward by filling with granulation tissue, by wound contraction drawing the edges inward, and by epithelialisation across the surface; it is slower and leaves a larger scar, as with an open abscess cavity or a pressure sore. Healing by tertiary intention, also called delayed primary closure, is a deliberate compromise: a contaminated wound is left open for a few days so that inflammation can settle and any infection declare itself, and is then sutured closed once it is clean — combining the safety of leaving a dirty wound open with the neat result of primary closure. Choosing among these is a core surgical judgement: a clean wound is closed primarily, a heavily contaminated or infected wound is left to heal by secondary intention or managed by delayed primary closure.
Provided image
- Primary intention: clean wound, edges apposed (sutured); fast, minimal granulation, neat scar.
- Secondary intention: wound left open (tissue loss/contamination/infection); heals by granulation, contraction and epithelialisation; slower, larger scar.
- Tertiary intention (delayed primary closure): contaminated wound left open a few days, then sutured once clean — safety of open management with a tidy final closure.
SELF-CHECK
A heavily contaminated traumatic wound is deliberately left open for four days and then sutured closed once it appears clean and free of infection. Which type of healing does this describe?
A. Healing by primary intention
B. Healing by secondary intention
C. Healing by tertiary intention (delayed primary closure)
D. Regeneration without scarring
Reveal Answer
Answer: C. Healing by tertiary intention (delayed primary closure)
Leaving a contaminated wound open for a few days to let infection declare and settle, then closing it surgically, is healing by tertiary intention or delayed primary closure. Primary intention closes a clean wound immediately; secondary intention leaves the wound open to granulate to completion.