Page 2 of 14
SU5.1-2 | Wound Healing and Wound Assessment — SDL Guide (Part 2)
Mechanisms: How Local and Systemic Factors Impair Healing
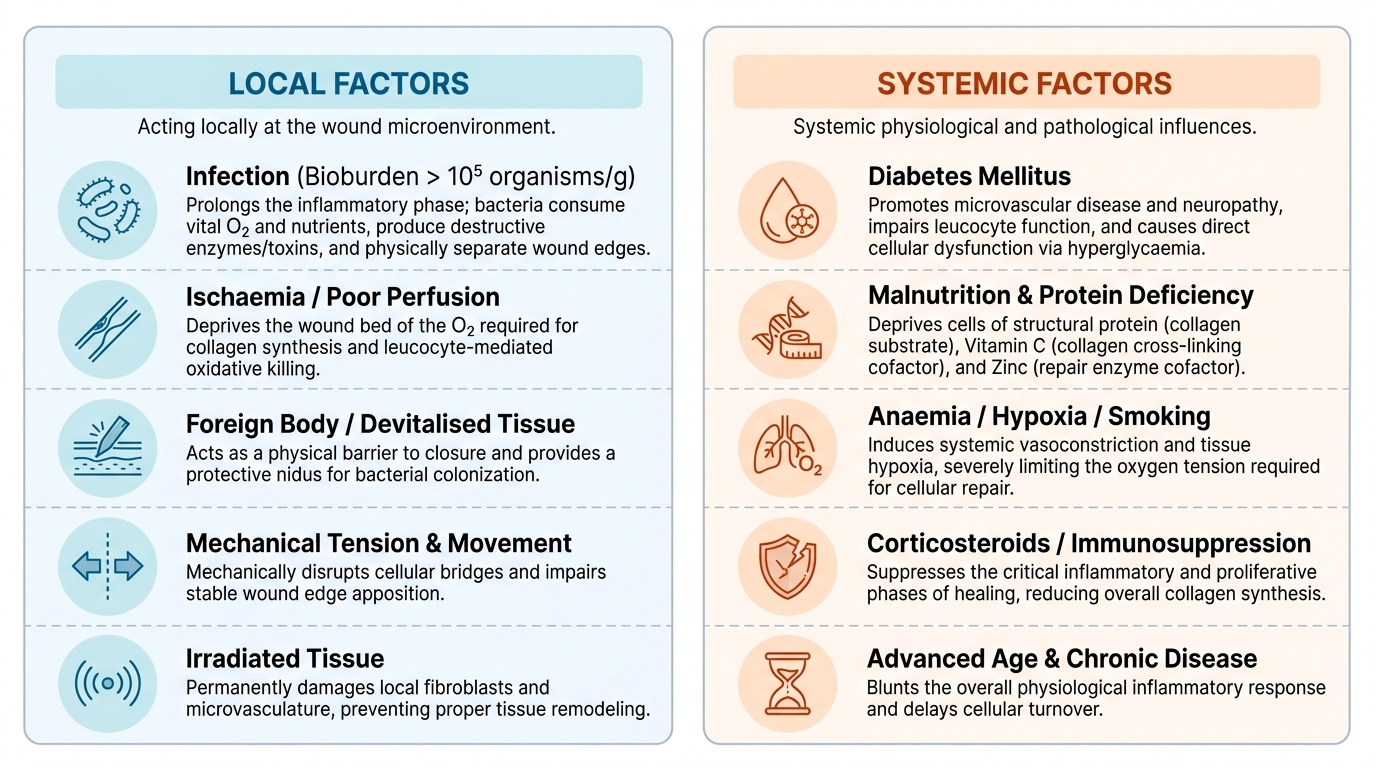
Healing fails when one or more of its phases is starved of what it needs, and the factors responsible divide cleanly into local factors acting at the wound itself and systemic factors acting on the whole patient. Among local factors, the most important is infection: bacteria consume oxygen and nutrients, prolong the inflammatory phase, produce destructive enzymes and toxins, and physically separate healing edges, so a wound with more than about 10^5 organisms per gram of tissue will not heal until the bioburden is controlled. Ischaemia and poor perfusion deprive the wound of the oxygen that collagen synthesis and leucocyte killing both require — hence the poor healing over pressure areas and in peripheral vascular disease. A retained foreign body or devitalised (dead) tissue acts as a nidus for infection and a mechanical barrier, which is exactly why surgical debridement matters. Mechanical tension across a wound and movement also impair apposition, and previously irradiated tissue heals poorly because radiation damages the small vessels and fibroblasts. Among systemic factors, diabetes mellitus is foremost, impairing healing through microvascular disease, neuropathy, impaired leucocyte function and the direct effect of hyperglycaemia. Malnutrition removes the substrate for repair — protein for collagen, vitamin C as the cofactor for collagen cross-linking (its lack, scurvy, causes wounds to break down) and zinc as a cofactor for the enzymes of repair. Corticosteroids and immunosuppression suppress the inflammatory and proliferative phases and reduce collagen synthesis (an effect vitamin A can partly counter). Smoking causes vasoconstriction and tissue hypoxia, while advanced age, jaundice and uraemia each blunt the response. The practical message is that most of these systemic factors are modifiable, and optimising them — glycaemic control, nutrition, stopping smoking — is genuine surgical treatment.
Provided image
| Group | Factor | Mechanism by which it impairs healing |
|---|---|---|
| Local | Infection | Prolongs inflammation, consumes oxygen/nutrients, releases destructive enzymes, separates edges |
| Local | Ischaemia / poor perfusion | Deprives wound of oxygen needed for collagen synthesis and leucocyte killing |
| Local | Foreign body / devitalised tissue | Nidus for infection and mechanical barrier; needs debridement |
| Local | Tension and movement | Disrupts apposition of edges |
| Local | Irradiated tissue | Damaged small vessels and fibroblasts heal poorly |
| Systemic | Diabetes mellitus | Microangiopathy, neuropathy, impaired leucocyte function, hyperglycaemia |
| Systemic | Malnutrition (protein, vitamin C, zinc) | Lacks substrate and cofactors for collagen synthesis and cross-linking |
| Systemic | Corticosteroids / immunosuppression | Suppress inflammation and fibroblast/collagen synthesis |
| Systemic | Smoking | Vasoconstriction and tissue hypoxia |
| Systemic | Advanced age, jaundice, uraemia | Blunted overall healing response |
SELF-CHECK
A malnourished patient with deficiency of a specific vitamin develops wounds that fail to heal and old scars that break down, because the cofactor needed to cross-link collagen is missing. Which deficiency is this?
A. Vitamin A deficiency
B. Vitamin C deficiency
C. Vitamin K deficiency
D. Vitamin D deficiency
Reveal Answer
Answer: B. Vitamin C deficiency
Vitamin C (ascorbic acid) is the cofactor for the prolyl and lysyl hydroxylase steps of collagen cross-linking; its deficiency (scurvy) impairs new collagen formation and causes old scars to break down. Vitamin K affects coagulation, and vitamin A can partly counter the healing impairment of corticosteroids.
Clinical Application: Eliciting and Documenting a Wound History
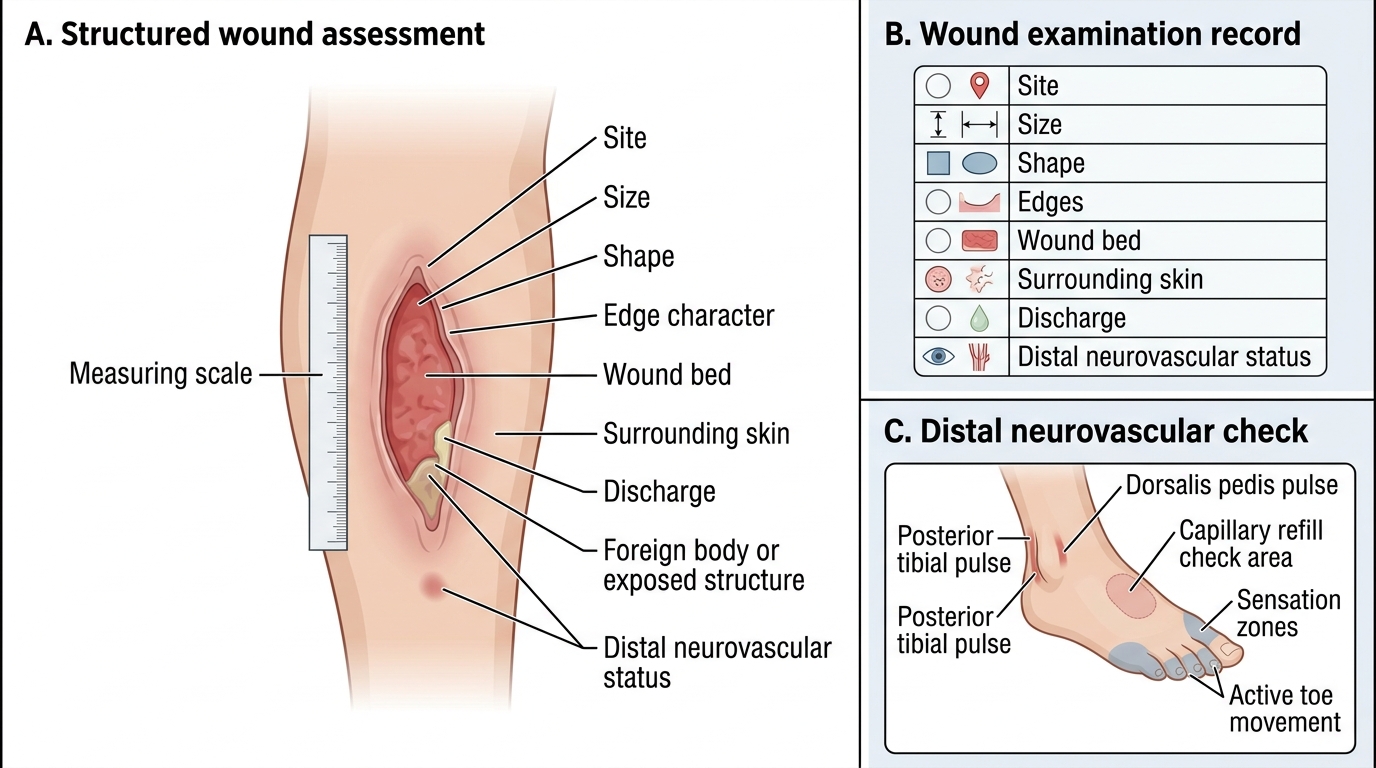
Understanding the biology is only useful if it is translated into a disciplined clinical assessment, and competency SU5.2 requires you to be able to elicit, document and present the history of a patient with a wound. Begin with the history of the wound itself: when and how it occurred (the mechanism — sharp, blunt, crush, bite, burn, or a surgical incision), the time elapsed since injury (which guides infection risk and closure decisions), the environment and degree of contamination (soil, water, faecal), and any first aid or treatment already given. Ask about symptoms — pain, bleeding, discharge and its nature, and any spreading redness, swelling or fever that would suggest infection. Then take a focused systemic history aimed squarely at the factors that impair healing: diabetes and its control, nutritional state and weight loss, smoking, alcohol, steroid or immunosuppressant use, peripheral vascular disease, and — critically for any breached skin — the patient's tetanus immunisation status. On examination, describe the wound systematically: its site, size (length, width, depth) and shape; the edges (clean, ragged, bevelled, undermined); the wound bed (healthy red granulation, slough, or black necrotic eschar); the surrounding skin (cellulitis, induration); the presence of discharge, foreign material or exposed deeper structures such as tendon or bone; and the distal neurovascular status. Finally, document all of this precisely and contemporaneously — accurate, dated wound notes and, where relevant, a diagram or photograph form the factual record on which both clinical management and any later medico-legal question depend.
Structured Clinical Assessment of a Wound
- Wound history: mechanism, time since injury, contamination, first aid given, symptoms (pain, bleeding, discharge, spreading redness/fever).
- Systemic history of healing factors: diabetes, nutrition, smoking, steroids/immunosuppression, vascular disease, tetanus status.
- Examination: site, size, shape, edges, wound bed (granulation/slough/eschar), surrounding skin, discharge, foreign body/exposed structures, distal neurovascular status.
- Documentation: precise, dated notes plus diagram/photograph — the factual record for management and medico-legal purposes.
Check Your Understanding
Before moving on, consolidate the model by reasoning through it rather than recalling isolated facts. Return to the diabetic, malnourished smoker from the start of this module whose incision broke down. Trace why: his inflammatory and proliferative phases are blunted by hyperglycaemia and impaired leucocyte function; his collagen synthesis lacks substrate and cofactors because he is malnourished; and his tissue oxygenation is reduced by smoking-induced vasoconstriction and microvascular disease — three systemic factors stacking onto one wound. Now test yourself on three links. First, can you name each of the four phases of healing in order and the dominant cell or event of each? Second, given a clinical wound, can you state whether it should heal by primary, secondary or tertiary intention and justify the choice? Third, presented with a slow-healing wound, can you list the local and systemic factors you would look for and explain the mechanism of each, then say which are modifiable? If you can take and document a structured wound history that systematically captures these factors, you have met both competencies. The short questions below check exactly these links.
CLINICAL PEARL
Never close a wound you have not satisfied yourself is clean. A contaminated or devitalised wound sutured shut traps bacteria and dead tissue and reliably abscesses; the safe path is thorough debridement and either healing by secondary intention or delayed primary (tertiary) closure once it is clean. And for every breach of the skin, ask one question that is easy to forget in the heat of a busy casualty: what is the patient's tetanus immunisation status?