Page 10 of 17
SU10.4 | Basic First Aid, Suturing and Minor Procedures — SDL Guide
Learning Objectives
- Describe the governing principles of basic first aid (the ABCDE primary survey and haemorrhage control), local anaesthesia with its maximum safe doses, suture and needle selection, and tetanus prophylaxis (SU10.4).
- Outline the technique of wound toileting, local anaesthetic infiltration, the simple interrupted suture and instrument tie, and abscess incision and drainage (SU10.4).
- Interpret a wound to decide primary, delayed primary or secondary closure, and perform these basic surgical skills in a simulated environment (SU10.4).
INSTRUCTIONS
First aid, wound care and basic suturing are the surgical skills you are most likely to use first and most often — at the roadside, in the emergency department, in any clinic. They save lives and limbs, and done badly they cause infection, scarring and harm. This module gives you the principles (including the local-anaesthetic safe doses you must never exceed), the step-by-step technique, and the judgement of which wound to close and when — all to be practised on simulation models before you ever take them to a patient.
References
- Bailey & Love's Short Practice of Surgery, Basic Surgical Skills and Wound Management (textbook)
- SRB's Manual of Surgery, Wounds, Wound Healing and Suture Materials (textbook)
- Sabiston Textbook of Surgery, Wound Healing and Acute Care / First Aid (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A young man arrives in the emergency department with a deep forearm laceration, bleeding briskly. Around him, three different mistakes are waiting to happen. One junior reaches for a tourniquet before even trying firm direct pressure. Another, keen to make the wound painless, draws up far more lignocaine than is safe for the patient's weight — enough to risk a seizure and cardiac arrest. A third is about to close the dirty, six-hour-old wound tightly by primary suture, sealing infection inside. None of these is a failure of effort; all are failures of knowing the simple, safe rules — pressure first, the local-anaesthetic dose ceiling in milligrams per kilogram, and which wounds you must not close. Basic first aid and wound skills look humble, but they are where avoidable harm most often happens, and where getting the fundamentals right saves lives, limbs and faces.
WHY THIS MATTERS
These are the surgical skills with the widest reach: you will use first aid, haemorrhage control, wound toileting and suturing in the emergency department, on the ward, in clinics and outside hospital, far more often than any major operation. They are immediately life- and limb-saving — controlling a bleed, securing an airway, cleaning and closing a wound correctly — and they are unforgiving of ignorance: an overdose of local anaesthetic, a tightly closed contaminated wound, or a missed tetanus risk causes real harm. The local-anaesthetic maximum safe doses in particular are knowledge you must carry exactly, because an error is potentially fatal. These competencies are examined directly and practically. Mastering them now in simulation — the doses, the technique, the wound judgement — builds skills you will rely on from your very first clinical posting and throughout your career, in every specialty.
RECALL
Recall the foundations these skills draw on. From your asepsis learning, recall that minor procedures are done under aseptic technique — clean skin preparation, sterile instruments and a sterile field — because even minor wounds become infected if asepsis fails. From wound-healing physiology, recall the phases of healing (haemostasis, inflammation, proliferation, remodelling) and that healing is impaired by infection, ischaemia, foreign material and devitalised tissue — which is why wound toileting and debridement matter. From anaesthesia (AS), recall that lignocaine is an amide local anaesthetic and that adding adrenaline causes vasoconstriction that prolongs its action and raises its maximum safe dose, while bupivacaine is the most cardiotoxic agent. From microbiology, recall that Clostridium tetani is a spore-forming anaerobe that thrives in devitalised, contaminated wounds — the basis of tetanus prophylaxis. These principles underpin every step that follows.
Why Basic Surgical Skills Save Lives and Limbs
The indication for basic surgical skills is any acute injury or wound — which means they are needed constantly, in and out of hospital, by every doctor. First aid is the immediate care given to an injured or ill person before definitive treatment, aimed at preserving life, preventing deterioration and promoting recovery. Basic wound care and suturing is the cleaning, assessment and closure of wounds, and minor procedures such as the incision and drainage of an abscess are small operations done under local anaesthesia. The reason these humble-looking skills matter so much is that they sit at the point of greatest avoidable harm: an uncontrolled external haemorrhage, an obstructed airway, a contaminated wound closed tightly, a local-anaesthetic overdose, or a missed tetanus risk can each kill or maim, and each is preventable by applying simple, well-defined rules. They are also the surgical skills of widest application — used far more often than any major operation — and the entry skills on which more advanced surgery is built. Because the consequences of error are immediate and serious (a fatal local-anaesthetic toxicity, a limb lost to uncontrolled bleeding, a hand crippled by wound infection), these skills demand exact knowledge and disciplined technique, rehearsed in simulation before they reach a patient. The rest of this module sets out the governing principles — including the local-anaesthetic safe doses, suture selection and tetanus prophylaxis — the step-by-step technique, how to judge which wound to close, and how you will practise under supervision.
The Governing Principles: Wounds, Anaesthesia and Suture Choice
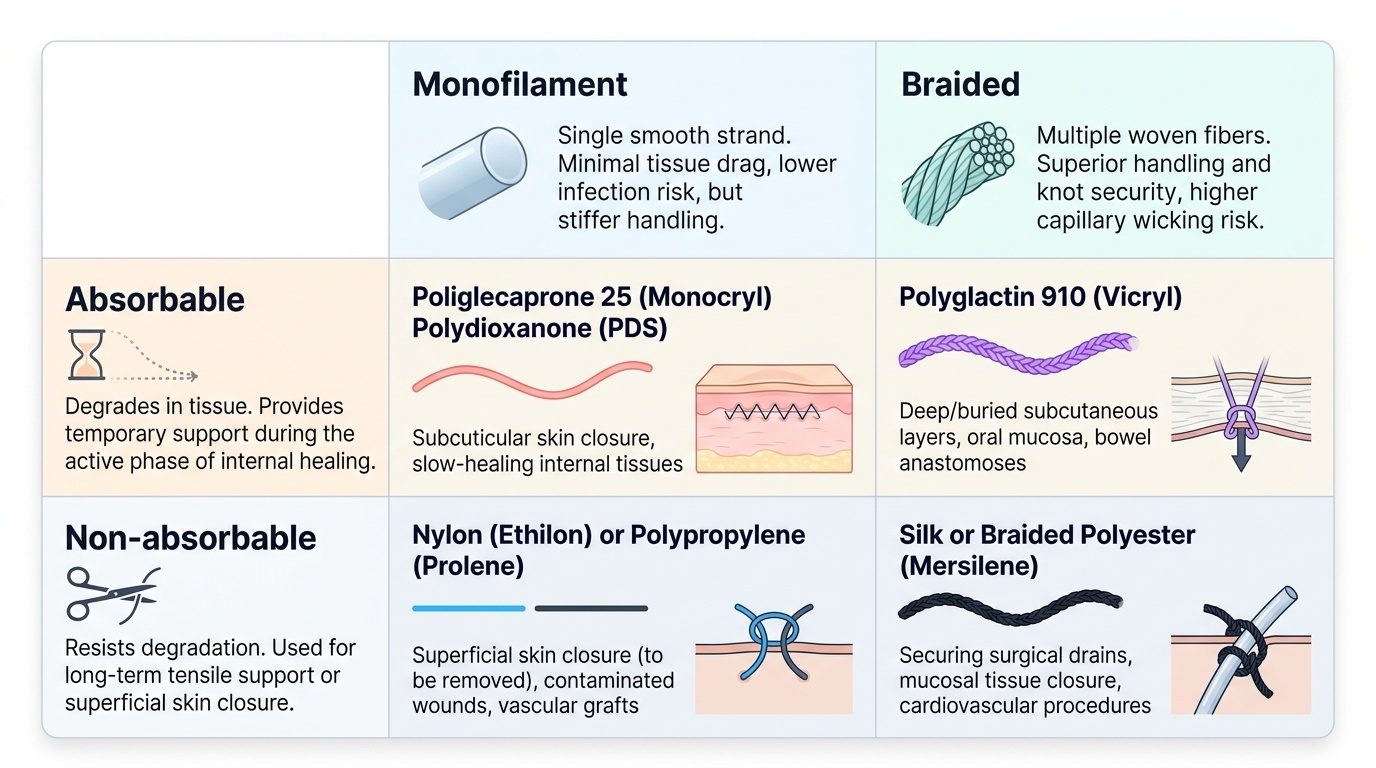
A handful of principles govern safe wound care, and the most safety-critical concern anaesthesia. The first principle is the primary survey: in any injured patient, assess and treat in the order ABCDE — Airway (with cervical-spine protection), Breathing, Circulation (including control of external haemorrhage), Disability (neurological status) and Exposure — because a life-threatening airway or bleeding problem must be addressed before a dramatic but non-fatal wound. The second principle concerns local anaesthesia and its maximum safe doses, which you must know exactly and calculate by weight: lignocaine 3 mg/kg plain and 7 mg/kg with adrenaline; bupivacaine 2 mg/kg (the most cardiotoxic agent — never give it intravenously or for intravenous regional anaesthesia). The adrenaline raises the lignocaine ceiling by causing vasoconstriction that slows absorption, and is classically avoided in end-arterial sites (fingers, toes, nose, ears, penis). Local-anaesthetic systemic toxicity (LAST) — perioral tingling and agitation progressing to seizures and cardiac arrest — is treated with 20% intralipid emulsion alongside resuscitation. Always quote the dose in mg/kg, never a fixed volume. The third principle is suture and needle selection: choose absorbable sutures (e.g. polyglactin/Vicryl) for deep, buried layers and non-absorbable (e.g. nylon, polypropylene) for skin to be removed later; prefer monofilament (less tissue drag, lower infection risk) for skin and contaminated wounds over braided materials (better handling but more capillary wicking); and use the right needle (curved, body-mounted) and gauge for the tissue. The fourth principle is tetanus prophylaxis: classify the wound as tetanus-prone (contaminated, devitalised, puncture, or more than six hours old) and give tetanus toxoid with or without tetanus immunoglobulin according to the patient's immunisation status. These principles are the safety scaffold for every wound you treat.
Provided image
| Category | Example | Typical use |
|---|---|---|
| Absorbable, braided | Polyglactin (Vicryl) | Deep/buried layers, mucosa |
| Absorbable, monofilament | Poliglecaprone (Monocryl) | Subcuticular skin closure |
| Non-absorbable, monofilament | Nylon, polypropylene (Prolene) | Skin (removed later), contaminated wounds |
| Non-absorbable, braided | Silk | Securing drains/tubes (high tissue reaction — avoid in skin) |
SELF-CHECK
For infiltration local anaesthesia, what are the maximum safe doses of lignocaine?
A. 1 mg/kg plain and 3 mg/kg with adrenaline
B. 3 mg/kg plain and 7 mg/kg with adrenaline
C. 7 mg/kg plain and 3 mg/kg with adrenaline
D. A fixed 20 mL regardless of body weight
Reveal Answer
Answer: B. 3 mg/kg plain and 7 mg/kg with adrenaline
Lignocaine maximum safe dose is 3 mg/kg PLAIN and 7 mg/kg WITH adrenaline — the adrenaline causes vasoconstriction that slows absorption and raises the ceiling. Doses must always be calculated in mg/kg by body weight, never as a fixed volume. Bupivacaine maximum is 2 mg/kg and it is the most cardiotoxic agent; local-anaesthetic systemic toxicity is treated with 20% intralipid.
The Technique: First Aid, Local Anaesthesia and Suturing
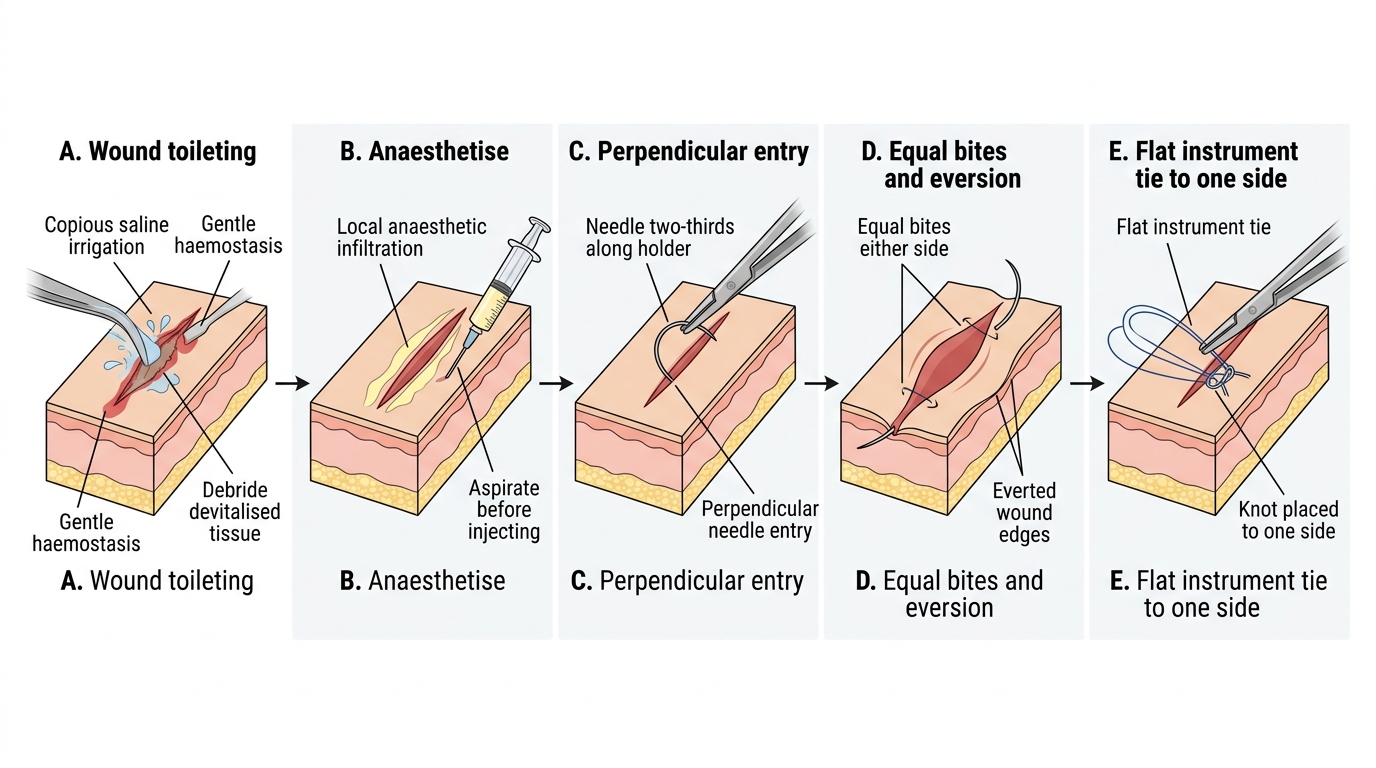
Each skill has a defined technique that you should be able to perform in sequence. In first aid for the injured patient, work through ABCDE: open and protect the airway, support breathing and give oxygen, and control circulation — the priority for an external bleed is firm, sustained direct pressure over the wound (elevate the limb; use a tourniquet only for catastrophic limb haemorrhage that direct pressure cannot control), then assess disability and expose to find all injuries while preventing hypothermia. For wound care, first achieve haemostasis, then perform wound toileting: clean the surrounding skin, irrigate the wound copiously (saline) to remove dirt and debris, and debride devitalised tissue and foreign material under aseptic technique, because dead tissue and contamination drive infection. To anaesthetise, draw up local anaesthetic within the calculated mg/kg limit, aspirate before injecting to avoid intravascular injection, and infiltrate the wound edges, waiting for the block to take. For simple interrupted suturing, mount the needle about two-thirds along its curve in the needle holder, pass it through the skin entering perpendicular to the surface, take equal bites of equal depth on each side so the edges meet without tension, gently evert the edges, and complete an instrument tie, laying the knot flat and to one side of the wound; place sutures evenly spaced. For abscess incision and drainage, under local or general anaesthesia make an adequate incision over the most fluctuant point, drain the pus, break down loculi, and leave the cavity to heal by secondary intention (often loosely packed) — never close an abscess cavity primarily. Throughout, maintain asepsis and dispose of sharps safely.
Simple Interrupted Suture: Step Sequence
- First aid: ABCDE — airway with C-spine, breathing/oxygen, circulation (direct pressure first; tourniquet only for catastrophic uncontrolled limb bleed), disability, exposure.
- Wound toileting: haemostasis → copious saline irrigation → debride devitalised tissue/foreign material, aseptically.
- Anaesthetise: within mg/kg limit; aspirate before injecting; infiltrate the edges and wait.
- Simple interrupted suture: needle two-thirds along the holder; enter perpendicular; equal bites; evert edges; flat instrument tie to one side.
- Abscess I&D: incise the fluctuant point, drain, break loculi, heal by secondary intention — never close primarily.