Page 11 of 17
SU10.4 | Basic First Aid, Suturing and Minor Procedures — SDL Guide (Part 2)
Interpreting the Wound: When to Close, When Not To
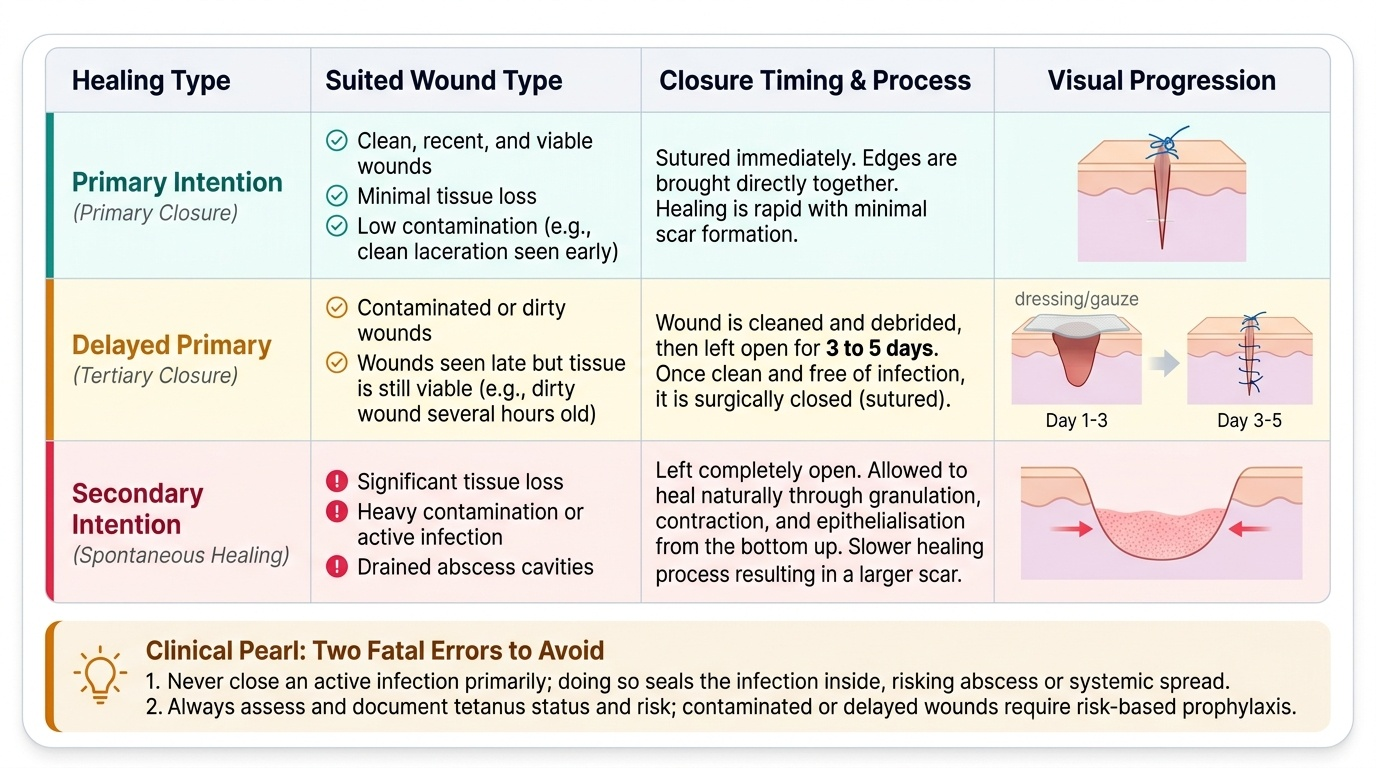
The judgement that separates safe wound care from harm is interpreting the wound to decide whether, and how, to close it. Read the wound against the type of healing you intend. Primary intention (primary closure) — suturing the edges together immediately — is appropriate for clean, recent, well-vascularised wounds with minimal tissue loss and low contamination (for example, a clean laceration seen early): healing is fast with a fine scar. Delayed primary closure is the safe route for wounds that are contaminated or seen late but viable (for example, a dirty wound several hours old): the wound is cleaned, debrided and left open for a few days, then sutured once it is clean and infection has not developed — closing such a wound primarily would seal infection inside. Secondary intention — leaving the wound open to granulate, contract and epithelialise — is for wounds with significant tissue loss, heavy contamination or established infection, and for drained abscess cavities; healing is slower with a larger scar but avoids trapping infection. Alongside this decision, always interpret the tetanus risk: a tetanus-prone wound (contaminated, devitalised, puncture, or more than six hours old) needs risk-based tetanus prophylaxis, and a heavily contaminated or high-risk wound in an inadequately immunised patient needs tetanus immunoglobulin as well as toxoid. Finally, read for features that demand referral rather than simple closure: wounds with possible tendon, nerve, vessel or joint involvement, deep hand and facial wounds, bites (high infection risk — usually not closed primarily), heavily contaminated wounds, and any wound beyond your competence. The interpretive rule is: match the closure to the wound's cleanliness and tissue viability, never close infection in, and escalate the complex wound.
Provided image
| Healing type | Suited wound | Closure timing |
|---|---|---|
| Primary intention | Clean, recent, viable, minimal loss | Sutured immediately |
| Delayed primary | Contaminated or late but viable | Cleaned, left open 3–5 days, then sutured |
| Secondary intention | Tissue loss, heavy contamination, infection, abscess cavity | Left open to granulate and contract |
CLINICAL PEARL
Two errors in this area can kill or maim, so carry the rules exactly. First, NEVER exceed the local-anaesthetic ceiling — lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline, bupivacaine 2 mg/kg — always calculated in mg/kg by weight, aspirating before you inject; local-anaesthetic systemic toxicity (perioral tingling → seizures → cardiac arrest) is treated with 20% intralipid. Second, NEVER close a contaminated, devitalised or late wound — or a drained abscess cavity — by primary suture: clean and debride it and use delayed primary or secondary closure, so you do not seal infection inside. And for any external bleed, firm direct pressure comes before a tourniquet — keep the tourniquet for catastrophic limb haemorrhage that pressure cannot control.
Performing the Skills in the Simulated Environment
The competency is demonstrated by performing these skills in a simulated environment under supervision, and simulation lets you build safe technique and judgement before any patient is involved. Practise first aid on manikins and scenario stations: run the ABCDE primary survey, control a simulated external haemorrhage with direct pressure and elevation, and articulate when a tourniquet is justified. Practise wound preparation on synthetic skin or models: irrigation, debridement and aseptic skin preparation. Rehearse the local-anaesthetic safety drill explicitly — state the patient's weight, calculate the maximum safe dose in mg/kg (lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline; bupivacaine 2 mg/kg), draw up within that limit, aspirate before injecting, and describe recognising and managing local-anaesthetic systemic toxicity with intralipid. On a suturing pad, practise the simple interrupted suture and instrument tie repeatedly — needle mounted correctly, perpendicular entry, equal bites, everted edges, flat knots, even spacing — and practise an abscess incision and drainage on a model, leaving the cavity open. Then run the judgement stations your facilitator sets: classify wounds and choose primary, delayed primary or secondary closure; decide tetanus prophylaxis from the wound type and immunisation status; and identify wounds needing referral. Throughout, maintain asepsis and safe sharps handling, and seek feedback on both technique and decision-making. Repeated supervised simulation is what makes the dose calculation automatic, the suture neat, and the wound judgement sound — so that when you treat a real injured patient, the safe habits are already in place.
Check Your Understanding
Consolidate the skill by walking from the injured patient to the closed wound. Start with first aid: the ABCDE primary survey, and for an external bleed, direct pressure first (tourniquet only for catastrophic uncontrolled limb haemorrhage). Then the principles: the local-anaesthetic maximum safe doses — lignocaine 3 mg/kg plain, 7 mg/kg with adrenaline, bupivacaine 2 mg/kg (most cardiotoxic), always in mg/kg, aspirate before injecting, LAST treated with 20% intralipid; suture selection (absorbable for buried layers, non-absorbable monofilament for skin and contaminated wounds); and tetanus prophylaxis for tetanus-prone wounds. Then the technique: wound toileting (irrigate and debride), the simple interrupted suture (perpendicular entry, equal bites, everted edges, flat instrument tie), and abscess incision and drainage healed by secondary intention. Then the interpretation: choose primary, delayed primary or secondary closure by the wound's cleanliness and viability — never close infection in — and refer complex wounds. Self-test on four links: can you state the lignocaine and bupivacaine maximum doses in mg/kg; can you say what comes first for an external bleed; can you match a wound to primary, delayed primary or secondary closure; and can you identify a tetanus-prone wound? The questions below check exactly these.
SELF-CHECK
A patient presents with a heavily contaminated, devitalised wound that is eight hours old but with viable surrounding tissue. What is the most appropriate approach to closure?
A. Immediate primary closure with interrupted sutures
B. Delayed primary closure — clean and debride, leave open a few days, then suture
C. Leave it entirely to heal by secondary intention with no intervention
D. Close primarily but give antibiotics to cover the contamination
Reveal Answer
Answer: B. Delayed primary closure — clean and debride, leave open a few days, then suture
A contaminated, devitalised, late but viable wound should undergo DELAYED PRIMARY closure — clean and debride it, leave it open for a few days, and suture once it is clean and uninfected. Immediate primary closure would seal infection inside. Antibiotics do not make primary closure of a dirty wound safe. This wound is also tetanus-prone (contaminated, devitalised, >6 h) and needs risk-based tetanus prophylaxis.